
Summary
In my latest post on March 26th I described a new Coronavirus group model, based on work I had done as a UK case study in support of a joint paper with lead author, Prof. Alex de Visscher, and with Dr. Tom Sutton, on “Second-wave Dynamics of COVID-19: Impact of Behavioral Changes, Immunity Loss, New Strains, and Vaccination” which has now been published for peer review as a pre-print on Springer’s site at https://www.researchsquare.com/article/rs-195879/v1.
This new model divides the UK susceptible population into four groups – 1) active/younger; 2) care-givers/mid-life; 3) vulnerable/older/at risk; and 4) school-going youth. This allows the different susceptibilities of these groups to Covid-19 to be coded into the model to help analyse the potential outcomes, given different parametric inputs to a theoretical model.
Some time ago, in my blog post on September 22nd, I discussed the age-dependency of risk to Covid-19 illness, with references to social mixing and the difficulty of isolating parts of the population from each other, as described in Adam Kucharski’s work.
Some Covid-19 aspects are dependent on such broad groupings, such as vulnerability to severe illness and death, and, in the UK, the prioritisation of vaccination of the community. Some mixing in the new model is allowed for by a cross-contamination factor between groups.
In that March 26th blog post, I had developed and fitted the model up as far as the January 3rd lockdown measures – Non Pharmaceutical Interventions (NPIs) – imposed in the UK, and this blog post brings the NPI status up to date, together with the future NPI relaxations intended, subject to progress, over the next few months.
I show that vaccination is key to our freedom to do this, and indicate the potential impact if such relaxations were considered in the absence of our UK vaccination programme, highlighting the importance of high levels of vaccination in eradicating the virus in all its variants.
I have also updated settings for differential mortality and propensity to serious disease between the four groups in the population.
Introduction
In the model I have used the latest UK vaccination progress figures, and the UK Government’s announced intentions for the near future regarding the priority groups for vaccination. I have updated mortality and infection characteristics for the four different groups: the fraction becoming seriously sick, fSS, and associated mortality, fmort.
This is in addition to the previous change to parameters for Group 4, school-age children, for whom I had already set these parameters very low, since UK evidence reflects very limited propensity for children to become seriously ill, as well as nearly zero death rate.
I have continued to include three variants – the first one from early in 2020; the second “Kent” variant from September 22nd 2020; and a putative third one, to represent a possible Brazil or South African variant, from January 1st 2021.
As with my previous modelling, the third variant doesn’t make a great impact in the vaccination model (UK257), since it arrives (into the model) when Non Pharmaceutical Interventions (NPIs) are already high and vaccination has just started to become effective.
Current “surge” testing in postcode areas of the UK where a small number of these “third’ variants have been found has indicated only hundreds of cases, and so the model’s indications are reflected in reality. As I write this post, it is reported that further urgent surge testing is under way in South London where more such cases have been detected.
Running the model without vaccinations (UK954), however, allows that third variant to grow sharply, showing the importance of maintaining UK progress in its vaccination programme. I show this in a later chart in the blog post.
In the vaccination scenario, I present charts for the overall comparison with published figures for cases and deaths, the contribution of the three variants, and also, utilising the group modelling, charts for each of the four population groupings.
I have added NPI relaxations for the start of the UK return to schools (March 8th); further relaxations of the current lockdown made on March 29th and April 12th; and the UK Government’s planned reductions of NPIs on May 17th and June 21st.
UK Population
Since a fundamental capability of the new model structure is to break the UK population down into age/vulnerability related risk groups, my starting point for the sizing of the groups is the following useful age group population presentation from Statistica:

Population groups in the new model
The total UK population in the model is 67.8 million, and utilising the population data above, I have defined the four groups, for this group model, fairly simply, adding some variation to the age bands to help represent more closely the priorities for vaccination. In my March 26th blog post, I weighted the % totals in each group to add to the known UK population total (since there is some overlap in the numbers when vulnerability aspects are taken into account) and I have continued to use these numbers.
| Groups | Name | Age range | Total | weighted % of 67.8m |
| 1 | Active/younger | 17-39 | 23.68m | 33.5% |
| 2 | Caregivers/mid-age | 40-64 | 21.25m | 30% |
| 3 | At risk | 65+ | 12.39m | 17.5% |
| 4 | School age | 0-16 | 13.42m | 19% |
Group mortality
As it is well documented that children suffer far less serious symptoms from Covid-19, and that mortality is far lower than for adults, I had already reduced mortality and serious sickness parameters for Group 4 in the model, school-age children, reported in my previous March 26th blog post. Other aspects of the role of children in transmission are not so clear.
My new changes for the fraction reaching Seriously Sick state (fSS), and mortality rate (fmort) for all groups are as follows in the table, and this time they are chosen, as a total weighted by the group populations, to be consistent with my previous average of 1.5% for fmort, the overall disease mortality rate for those falling sick, and 10% for fSS, the overall propensity of those falling sick to become Seriously Sick:
| Group | Description | % of population | Prior fSS | Prior fmort | New fSS | New fmort |
|---|---|---|---|---|---|---|
| 1 | Active/younger | 33.5% | 4% | .2% | 5% | .16% |
| 2 | Caregivers/mid-age | 30% | 10% | 1.5% | 12.6% | 1.17% |
| 3 | At risk | 17.5% | 20% | 8% | 25.2% | 6.26% |
| 4 | School-going | 19% | .5% | .005% | .6% | .004% |
| All | Weighted average by % pop | 100% | 7.9% | 1.92% | 10% | 1.5% |
Priority list and schedule for vaccination
My earlier modelling, reported in my recent blog posts, indicates how vital the vaccination programme is to allow NPIs to be reduced during 2021. The possibility for NPI relaxation closely mirrors the vaccine deployment, as shown in my blog post on February 12th, and which Alex, Tom and I covered in the paper referred above, to which I also referred in my latest blog post on March 26th.
“The outcome is that the vaccine programme in the UK has the potential to reduce the imposition of NPIs on March 7th by about 15%, without costing lives, this being the next time we in the UK are due for a major NPI review, potentially involving the return of schools at around March 7th.“
Thus a key corollary to the population data is the UK Government’s current and published vaccination schedule, which I reflect in data for the new model, together with the vaccination rates and changes of vaccination efficacy, and the UK Government’s announced NPIs.
The Government decided to focus more on first inoculations, delaying planned second inoculation beyond the three weeks interval originally envisaged (and approved by the UK Regulatory Agency) to a maximum of twelve weeks. Most authorities around the world have supported such a move in principle, to help protect more people as soon as possible, since first doses were shown to confer reasonable protection.
The University of Sheffield reported their study with other Universities, including Oxford University and the University of Liverpool, which found that 99 per cent of people generate a robust immune response against Covid-19 after just one dose of the Pfizer vaccine.
The study’s findings were also that people who had previously been infected with the virus achieved extended immunity after one dose. This should encourage the take-up of the second, booster vaccine dose to achieve an enhanced effect.

Soon after this list was announced, the Government published further details about the schedule for some of these groups:
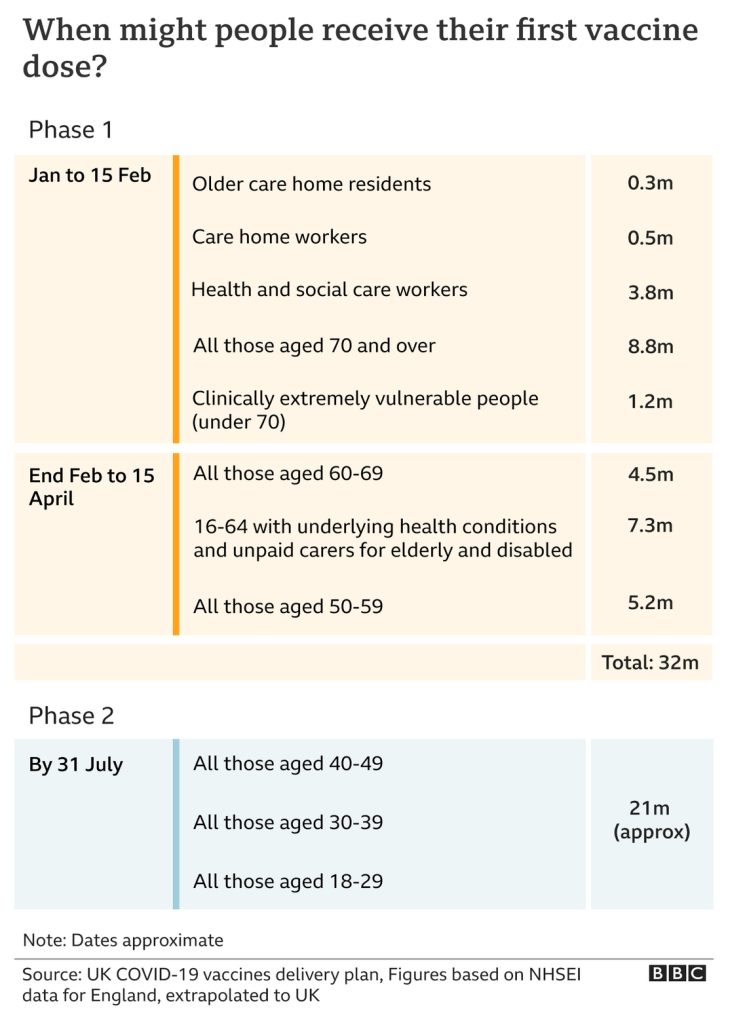
The UK Government vaccination website reports that the vaccination programme is still on track, with the efforts during April more focused on second vaccinations for the more vulnerable groups. Over 30 million first doses have already been dispensed as I write this, with a further 7.5 million second doses dispensed, nearly 40 million first and second doses in all.

As the BBC said in mid-April for those second doses:
The serious illness and death rates from Covid-19 for children are very small, and there is no UK approval yet for the vaccination of children, as reported in The Times in August 2020 (at a time when the second and third waves of infection had not yet been suspected). I have therefore scheduled no vaccinations for school-age children (Group 4 in the model), utilising the group structure I describe below.
Vaccination schedule in the group model
I increased the number of stages of vaccination in the model on March 26th to reflect information that the UK Government has published about its intentions and priorities regarding the first dosing schedule, the achieved rates, and the typical efficacy of the vaccines as reported from studies on antibodies stimulated by vaccines, including for different variants. Reported cumulative vaccination rates to date (April 11th 2021) for first and second doses are:

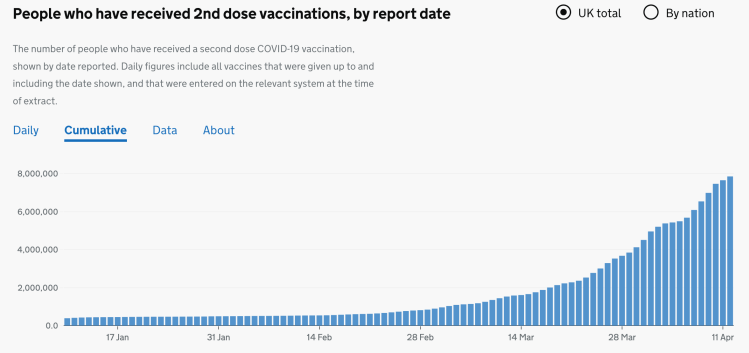
The situation we faced in April regarding reduced first vaccination rates is a product both of the desire to progress second doses, which, as we see, are already beginning to increase, as well as the well-publicised issues with vaccine supply from Europe and India. Fortunately most of the vaccine production for British patients is based in the UK, at least for the AZ Oxford vaccine. Additional vaccines such as Moderna and Novavax will be available later this year.
| Model Day | Date from: | Vaccinations per day | Efficacy | Groups |
|---|---|---|---|---|
| 335 | January 1st | 300,000 | 70% | Group 3 at risk only |
| 366 | February 1st | 450,000 | 85% | Group 3 at risk only |
| 411 | March 18th | 500,000 | 85% | Groups 2 and 3 |
| 425 | April 1st | 300,000 (first doses) | 85% | Groups 2 and 3 |
| 455 | May 1st | 500,000 | 85% | Groups 2 and 3 |
| 486 | June 1st | 500,000 | 85% | Groups 1, 2 and 3 |
The available vaccinations from each date are shared between the listed groups in the table on a per capita basis. Group 4, school-aged children are not yet scheduled for vaccination, as mentioned before, as there is no UK approval for inoculating children with Covid-19 vaccines.
I have ignored second doses in the model for now, but I would approach that by increasing efficacy where required and by adding some extra vaccination rate change points in the schedule. I have not ventured to ascribe different efficacy to different vaccines (they seem quite similar at the moment), or to explore the possibly different vaccine efficacy against different variants. As you see from the table above, I reduced the April first doses in the model to reflect Government policy.
Non Pharmaceutical Interventions (NPIs)
For the 2020 history, I had previously chosen NPIs close to those I used for my previous reports, simplified where possible to reduce complexity. Some of them had been set to zero in the original model, as some had been ineffective in practice in the light of public response to them.
In the new model the NPIs and dates still correspond to step changes in the UK Government’s lockdown and easing measures, starting with the original lockdown on March 23rd 2020. In my previous post, the final data point for NPIs in the model on January 3rd 2021, and in this post I update the model with the UK Government 2021 NPI relaxations already made, and planned.
The changes to Mortality and Serious Sickness requires some changes to the model % NPIs to reflect the history to January 3rd. The new model NPIs are in some cases different for different groups; for example return to school affects predominantly school-age children. NPIs are shown here as averages* over the groups (although they can be, and in some cases are set individually for each group in the model) and are as follows, with any zero NPI changes left in for easier comparison with my previous posts:
| Day number | Date | Average NPI reduction* | Cumulative NPI status |
|---|---|---|---|
| 52 | 23/03/2020 | 86% | 86% |
| 155 | 04/07/2020 | -1.00% | 85% |
| 186 | 04/08/2020 | -4.00% | 81% |
| 197 | 15/08/2020 | -0.00% | 81% |
| 214 | 01/09/2020 | -16.00% | 65% |
| 227 | 14/09/2020 | 1.00% | 66% |
| 237 | 24/09/2020 | 3.00% | 69% |
| 270 | 27/10/2020 | -1.50% | 67.5% |
| 280 | 06/11/2020 | 12.5% | 80% |
| 306 | 02/12/2020 | -3.00% | 77% |
| 320 | 16/12/2020 | 0.00% | 77% |
| 327 | 23/12/2020 | -12.00% | 65% |
| 332 | 28/12/2020 | -2.00% | 63% |
| 335 | 31/12/2020 | -2.00% | 61% |
| 338 | 03/01/2021 | 26% | 87% |
| 401 | 07/03/2021 | -2.0% | 85% |
| 423 | 29/03/2021 | -5.0% | 80% |
| 437 | 12/04/2021 | -3.765% | 76.235% |
| 472 | 17/05/2021 | -3.765% | 72.47% |
| 507 | 21/06/2021 | -4.13% | 68.45% |
The % NPI effectiveness changes mean that the normal transmission rate of any virus variant (people infected per day by an infected person) is reduced by that % figure; thus the simulation’s first lockdown reduction of transmission rate is on March 23rd by 86%, which means that the transmission is reduced to 14% of its usual value. Negative NPI adjustments in the table reflect a % increase in NPI effectiveness.
Measures (NPIs) such as social distancing, shielding, working from home where possible, and/or all the rest of the measures enacted at any particular stage are represented in the model by different % changes in the model NPIs at those points of UK Government NPI changes, and public responses to them.
In this post, as promised before, I have addressed the return to schools on March 8th (already trailed in my February 12th blog post and further explored in the March 26th post) and incorporated several further projected easings of the lockdown in the Government’s planned schedule until Midsummer’s Day, 21st June 2021, when the UK Government has indicated that all legal restrictions might be removed.
Presumably this means, however, that advisory precautions will still be in place. Vaccine passports, and some quarantining for international travel seem likely to be required, with a traffic light system for categorising the risk of travel to and from other countries. Many measures adopted voluntarily by the UK population, such as social distancing and mask wearing indoors and/or in enclosed public places are also likely to continue. Thus my model NPIs do not reduce to zero at any point.
The UK Government has allowed itself an interval between each successive NPI change for analysis of the effectiveness (or otherwise) of the change, and reserves the right to adjust measures and their timing in the light of outcomes.
United Kingdom Reported Cases, active cases and deaths
The first chart 207 shows only reported data for the UK, up to April 11th, sourced from the Worldometers UK website.

We see the significant reduction in active cases during 2021, leading to flattening of the overall cumulative cases and deaths curves in recent weeks. I use this reported data in the following Chart 19 to compare with my model predictions.
Charts for the group UK simulation
The following chart 19 for model dataset UK955 shows the overall modelled progress of the pandemic in the UK, as at April 11th 2021, but with no 2021 NPI relaxations in the model. This Chart 19 compares the overall outcomes for active cases and deaths with the reported data above, with no NPI changes after January 3rd, Day 338, and indicates the good fit of the model to reported data up to that point.

The fit of the modelled pandemic for this grouped version isn’t quite as close as for my original model, which has been refined over many months, but there are many more parameters to set in the new model.
Instead of 16, the new model has 64 compartments, the term used for the health status sets of people in SIR models (at their simplest, the three compartment Susceptible-Infected-Recovered models that I described in my April 8th 2020 post) in different stages of health or illness. For four groups, and three variants, we have the following compartment classifications. In the charts, Active Cases comprise compartments I, S, SS and B, the currently infected individuals. All Cases comprise the Active cases plus R and D, Recovered and Deceased people, who have been infected at any prior point, but not Vaccinated or Uninfected people.
| Compartment | Description of compartments | How many |
|---|---|---|
| U | Uninfected/healthy for each group (4) | 4 |
| V | Vaccinated people for each group | 4 |
| R | Recovered people for each group | 4 |
| D | Deceased individuals for each group | 4 |
| I | Incubating infected people, one per variant (3) per group (4) | 12 |
| S | Sick infected people, one for each variant, per group | 12 |
| SS | Seriously Sick, one for each variant, per group | 12 |
| B | Better people (recovering), one per variant, per group | 12 |
| Total 8 | All modelled compartments | Total 64 |
For the time being, I won’t attempt to make the simulation even more accurate for the current data inputs, because I will continue to change input parameters, to fit emerging information. For example, Public Health England recently released more refined data on priority vaccination groups, as follows:
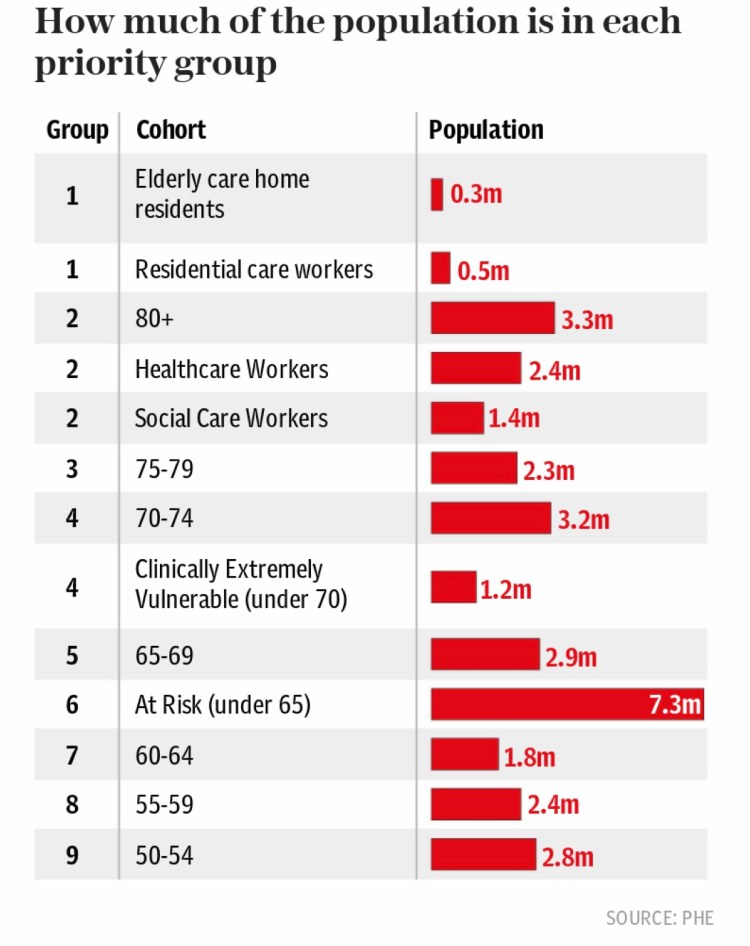
This would make a difference to the % of population within each of the four population groups, thus altering the balance of infectivity and therefore the outcomes, as displayed in Chart 19 above. It gives an idea as to the complexities of the modelling process, which now that I have finished programming the new model functionality, becomes as much a data analysis problem as a computer coding problem.
For this post I have focused on the fSS and fmort changes, and 2021 NPI changes.
Comparative case for 2021 NPI relaxations
In the next model scenario, I will run projections for 2021, addressing the following summary roadmaps for lockdown easing in England and Scotland, as examples of the approaches of the four home countries in the UK to reducing NPIs over the next few months.

England’s lockdown easing roadmap 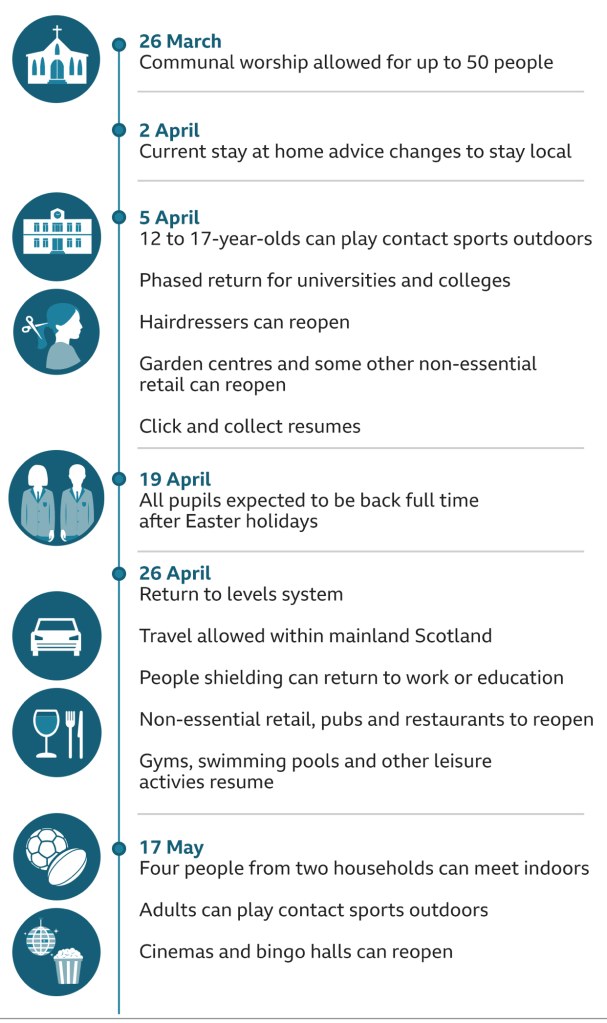
Planned lockdown easing schedule in Scotland
Such easing programmes, hopefully, are what vaccination will allow us to do without allowing SARS-Cov-2 prevalence to grow again.
Epidemics, and their models, have the propensity to become cyclical, as restrictions are imposed and removed, and then reimposed, as I showed in one of my earlier posts, and vaccination was always going to be the way to break that cycle, as I said in that post, and in others.
My next Chart 19 shows the projected outcome with the NPI relaxations for the March 7th return to schools, and for the four dates shown in the table above, March 29th, April 12th, May 17th and June 21st. These latter dates (i.e. after the March 8th return to schools) are the most critical, involving, as they do, quite large reductions in NPIs for most groups of people. The vaccination programme, Vac1 to Vac6 over six dates, as discussed above and annotated in the chart, is now in place in the model dataset UK957.

We see that compared with the UK955 case for no 2021 NPI relaxations, the UK957 model responds with c. 10,000 extra deaths (137,385 minus 127,512) over the next 12 months or so. This indicates the ever-present danger of the SARS-Cov-2 virus reasserting itself, possibly through the growth of the third variant which I have postulated in the model with double the infectiousness of the first variant (remember the second “Kent” variant is 70% more infective in the model). All variants have the same mortality fmort and propensity to Serious illness, fSS at present, although these key parameters can be changed in the model.
This is just a model, and the purpose here is to look at the sensitivities of such model to many of the characteristics of virus variants, Government NPI responses and public behaviour, and vaccination rates and efficacies. The data to fulfil such a model is complex, and many interdependent data items can be changed and affect outcomes in different ways. The same outcomes can be achieved by different changes, and so care must be taken in interpreting model projections, understanding which changes are causing which effects. This, in many ways, is why we run models at all.
Prevention of transmission by vaccinated people
I have added model functionality to represent the different (probably lower) efficacy of vaccines in preventing transmission of infection from vaccinated people. I am convinced this will be necessary if such efficacy is much lower. There is an argument that community “herd” immunity is harder to reach if the vaccines aren’t good at preventing such transmission, even though they are highly effective at reducing severity of disease in those vaccinated.
The argument on this was well presented at a surprising source, where Matthew Woodruff, an immunologist at Emory University, Atlanta, US, is quoted as saying: “IgG antibodies act as thugs that react swiftly to all kinds of bacteria and viruses. But while they make up the bulk of our antibodies, they’re confined to our inner organs, such as muscles, blood and the lungs. But we also have another kind of antibody produced by our immune system, antibodies that deal with invaders as they enter the body from the outside and it could be even more important.
“Spaces like the nose, the throat, the lungs and digestive tract rely on another antibody, immunoglobulin A, or IgA antibodies. As yet, we don’t know how vaccines incite IgA antibodies that protect you as you breathe, eat, drink and touch your face. As the result of a Covid infection, your body manufactures huge amounts of these more-specialised IgA antibodies. Because they’re on the same respiratory surfaces that transmit coronavirus, it’s logical to assume people who recover from Covid aren’t spreading it any more.
It will probably take years for research to reveal how well vaccines can prevent Covid transmission.
But there’s another yardstick to tell if a vaccine is stopping a person from transmitting it. Community spread – the number of new cases. If numbers are rising, the virus is being passed on, if they’re falling, it isn’t spreading. Vaccines are working.
“I can’t imagine how the vaccine would prevent symptomatic infection at the efficacies that trials reported and have no impact on transmission.”
So we’ll have to wait to know for certain if people who got the vaccine can still transmit the virus, and if so, by how much compared to unvaccinated people.
Further work is being undertaken – “Project S” – as an entire town is vaccinated as experts race to understand if Covid jabs halt transmission.
In the study, known as a “stepped-wedge cluster randomised trial” in scientific jargon, the town, Serrana in in São Paulo state in Brazil, has been split into 25 areas. Vaccinators will immunise all adults in one area before moving to another, allowing researchers to compare infection rates in neighbourhoods that have and haven’t received the jab. Change over time will also be analysed – enhanced surveillance has been in place in Serrana since September.
“In general, a cluster trial is best placed to evaluate [the] impact of vaccination on transmission,” Dr Adam Kucharski, an infectious disease epidemiologist at the London School of Hygiene and Tropical Medicine who is not involved in the study, told The Telegraph.
“The vaccine both protects individuals within the cluster because they’re vaccinated (the ‘direct’ effect) as well as protecting them because transmission is reduced (the ‘indirect’ effect).”
But he cautioned against comparing results from different trials, as they have different parameters, and warned that just because one vaccine is found to prevent coronavirus transmission does not mean they all do.
Comparative charts for the different risk groups
The benefit of the group model is to help understand in more detail the different outcomes for the different risk groups in the model. The slideshow below compares the 4 individual group outcomes, together with the total population outcome across all groups, for the UK957 dataset. Remember there are no vaccinations for school age children (Chart 24), and also that Group 1 (young/active, Chart 21) vaccinations don’t start until the sixth Vaccination rate change date at 1st June 2021, with Group 2 (Carers mid-age, Chart 22) starting on 18th March 2021. Only Group 3, at risk/vulnerable/older, are vaccinated from the outset, January 1st, representing the approximate date at which the vaccinations originally begun in the UK on December 8th become effective.



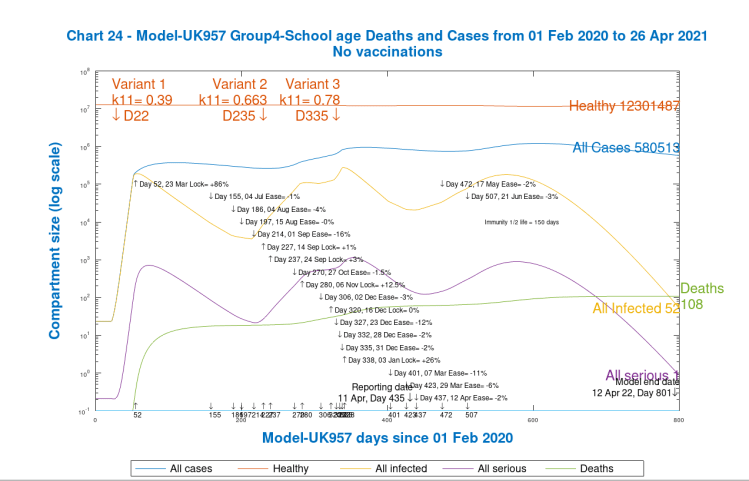
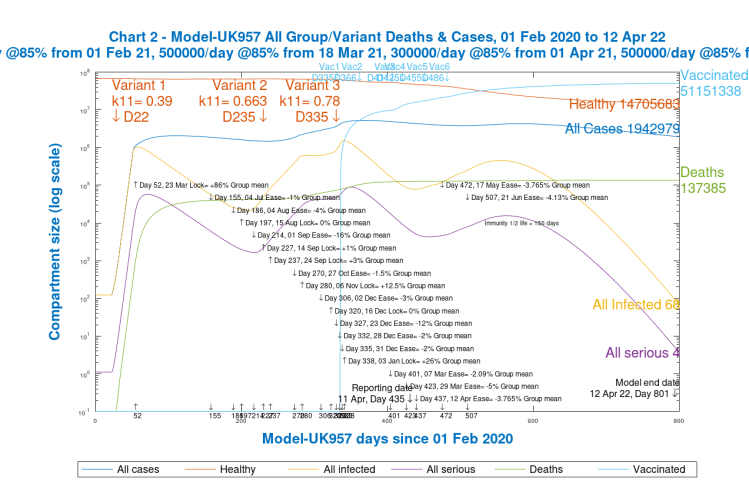
Even with the very low fSS and fmort I have set for school-age children, 108 deaths (on Chart 24) is too high, but I can address this with further settings next time. Overall the model outcomes exhibit the right kind of relationship between the outcomes for different risk groups, adding up to something that looks like the UK national observed situation (chart 2 in the slideshow here, and Chart 209 below).
By now you will understand that there are lots of adjustable parameters in the model. I probably need a research team to source all the data that is needed!
The role of the different variants
I have three variants in the model, as stated in the introduction. The first starts at the beginning of 2020; the second “Kent” variant that was thought to start in the south-east of England, starting on September 22nd (when it was first taken from a swab, and analysed later); and also a “placeholder” third variant that might stand for an incoming Brazilian or South African variant. It is possible in the model to add as many as we wish. The following timetable for the detection of the “Kent” variant, and its growth to dominate the UK case numbers, shows why the UK Government is being so careful about new variants now, restricting international travel for leisure purposes so tightly, making it illegal with severe penalties.
The analytical confirmation of a new variant is some weeks behind its arrival. To be ahead of it, proactive restrictions have been set on travel to and from places where new variants have been seen or are suspected.

The variant characteristics in the model are:
| Variant # | Model day | Start date | Transmission rate | Infection prevention* |
|---|---|---|---|---|
| 1 | 22 | Feb 1st 2020 | 0.39 | 67% |
| 2 “Kent” | 235 | Sep 22nd 2020 | .663 | 67% |
| 3 | 335 | Jan 1st 2021 | .78 | 67% |
The transmission rate figure 0.39, for example, means that an infected person would infect 0.39 people/day if no NPIs are in place to restrict normal interactions.
*The Infection prevention parameter (67% in table) is available but unused in the model at present, but would reflect the vaccine capability to prevent infection with the variant from vaccinated people.
The transmission rate for the second variant is at the top end of the confidence interval suggested by a January study for its assessed transmission rate. The third variant’s transmission rate (unilaterally attributed by me) is not so important for the model at the moment, because, as we see below, in the vaccination model, the variant fails to takes off because it arrives into the model when model NPIs are already quite high, and vaccination has already started.
Variant development comparisons
I now present chart 303 for the Group model dataset UK957, showing the growth and decline of all three variants for the whole population, in the context of both the vaccination programme underway in the UK, and the 2021 NPI relaxation programme.

Note that in the model (as with others in this blog post) I have set the half-life of immunity to at 5 months (150 days), in line with a recent analysis of waning immunity.
There is likely to be a policy of vaccination booster updates in the future, possibly on an annual basis if the rate of immunity decline allows. Infectivity of vaccinated people is set at zero in both models at present, although as stated, the most frequent assessment I have seen so far is that vaccines are only 67% effective in cutting transmission from vaccinated people.
In the model we see that the second variant becomes very important, as experienced by most countries, especially the UK, where that variant, or ones like it (variants do share some common characteristics) have appeared. It wasn’t publicised in the UK until late November, although it was present from September 22nd as evidenced by later analytical results from swabs taken then.
As a result of this experience, “surge” testing in some UK postcodes, where the Brazilian or South African variant has appeared in small numbers, has been initiated to control the growth of those potentially damaging variants, to avoid any surge in infections. There also remains concern that one or other of the variants might be more resistant to vaccines.
In an effort to control the spread of coronavirus variants, the London Boroughs of Hillingdon, Lambeth, Wandsworth, Southwark and Barnet have all just announced testing and contact tracing. Sandwell council in the West Midlands has also announced it will undertake surge testing.
This is why I have the third variant in the model as a place-holder for a variant such as the Brazilian or South African one, although there are many variants appearing all around the world now. The model can cope with as many as are needed. A recent article by Jane Merrick of the Independent provides a useful checklist of such variants, with some of their key characteristics. The UK Government website here also lists Variants under Investigation (VuIs) and Variants of Concern (VoCs), a surprisingly long list.
As the Times newspaper reported, there is new concern over a variant that has been seen in India, VUI-21APR-01, and now also in a few cases in the UK. There have been 77 cases of the strain, known as B.1.617, recorded in the UK up until April 14, according to Public Health England (PHE). Statistics show 73 cases were recorded in England and four in Scotland. It has worried some experts because it contains two mutations in its spike protein that, it has been suggested, may boost its ability to escape the body’s immune responses. It is thought the variant may also be able to infect the body more easily than other strains.
Prof Paul Hunter, professor in medicine at the University of East Anglia, said the arrival of the India variant was potentially worrying. “These two escape mutations working together could be a lot more problematic than the South African and Brazilian variants who have only one escape mutation,” he told The Guardian. “It might be even less controlled by vaccine than the Brazilian and South African variants.”
Variants under investigation are listed at this UK Government PHE website, including the new India variant VUI-21APR-01.
Differential mortality of variants in the model
The model can set fss and fmort differently for each variant. Back in January, there had been some suggestion that as well as being it to 70% more infective, the 2nd “Kent” variant might be 30% more lethal, but a new Public Health England study is reported as saying “a 34% increased risk in hospitalisation associated with the [Kent] variant compared to wild-type cases” which suggested “increased infection severity associated with this variant. However, no significant difference in the risk of mortality was observed”.
But prior studies had found increased mortality and hospital admission rates, as the report says. I will make further changes once there is more definitive information.
A lot has been learned about the virology of SARS-Cov-2 over the last 12 months, but there is clearly more to learn about the variants that are appearing, and about any common characteristics they might share, especially regarding any differential effectiveness of vaccines against them. It is hoped that the more recent mRNA (modified RNA) technique of vaccine development, as well as fast-tracked approval processes, will allow faster responses to new strains of the virus.
What if there had been no vaccination?
As a very worst case scenario, I present a version of Chart 303, for model settings UK954, where there is no vaccination, but NPI relaxations have gone ahead anyway. In this case, we see that although variant 1 has declined completely by the 800 day point (April 12th 2022), Variant 2 (the “Kent” variant) remains dominant, and also that the third variant thrives, leading to the epidemic spiralling out of control at these model settings.
This scenario isn’t realistic, because a) there is a vaccination programme, and b), no Government would relax NPIs to such an extent in these circumstances. But I have these variants and options in the model to explore and calibrate as test cases. It does tend to highlight, however, the vital role that vaccination is playing in controlling the epidemic.

We see both the second and third variants in the model are still increasing at 800 days, with large numbers of active cases and serious cases at that point. This is in direct contrast to the preceding vaccination model UK957, where all the variants have been snuffed out by the high level of vaccinations, 51 million across the three adult groups at the 800 day point.
Bear in mind that the model doesn’t vaccinate the 12m school-age children in Group 4 in the model at any stage (19% of the UK population in the model), and so 51m vaccinated in model UK957 represents vaccination of a very high proportion of the intended target population of 67.8m x 81% = 55m. 51m represents, therefore, about 93% of those intended to be vaccinated in the model.
Outcomes for the older and vulnerable population
The UK Prime Minister reportedly suggested that lockdown was primarily responsible for the sharp decline in UK cases and deaths in the last three months. It is hard to say why this would be said, since it is everyone’s interests that the public both comply with NPIs and get the vaccine when offered, and both are playing a part.
A paper published by academics from several Universities (the London School of Hygiene and Tropical Medicine (LSHTP), Imperial College and the University of Strathclyde) with Public Health departments in all four home UK countries, makes clear the beneficial effect of the vaccination programme for adults over 70.
They concluded in the abstract “Vaccination with either a single dose of BNT162b2 or ChAdOx1 COVID-19 vaccination was associated with a significant reduction in symptomatic SARS-CoV2 positive cases in older adults with even greater protection against severe disease. Both vaccines show similar effects. Protection was maintained for the duration of follow-up (>6 weeks). A second dose of BNT162b2 provides further protection against symptomatic disease but second doses of ChAdOx1 have not yet been rolled out in England. There is a clear effect of the vaccines against the UK variant of concern.’
Model outcomes for older and vulnerable people
My model also confirms the vaccination benefits for older people, and here I present charts for datasets UK955 (vaccination) and UK953 (no vaccination) for Group 3, the at risk group including older people. Firstly, without 2021 NPI relaxations in either case:


We see a clear difference in model outcomes, with vaccinations saving 15,909 lives (107,634 – 91,725) in this group at 800 days (April 12th 2022).
This seems the right order of magnitude (for a longer period) compared with the UK Government view that vaccination has saved 10,400 lives of older people already, as reported by Public Health England. Their own chart in that report shows this clearly:

Their report states “By the end of March 2021, it is estimated that 9,100 deaths were averted in individuals aged 80 years and older, 1,200 in individuals aged 70 to 79
and 100 in individuals aged 60 to 69 years giving a total of 10,400 deaths averted in individuals aged 60 years or older.”
I have run model Group 3 (at risk, vulnerable & older) analysis for the case with the 2021 NPI relaxations, as a comparison using datasets UK957 (with vaccinations) and UK953 (no vaccinations), the latter case where the model responds with a similar runaway situation as for the overall outcome presented in chart 303 in the previous section.
I emphasise again that UK953 is an unrealistic scenario because a) there is a vaccination programme, and b) if there were no vaccinations, the UK Government could not embark prudently on such an NPI relaxation programme.

We see that NPI relaxations in the vaccination case UK957 make a difference of an additional 2,156 deaths (93,881 – 91725) by Day 800 compared with the prior UK955 ‘no relaxation’ vaccination case above. For this most vulnerable group, the ‘no vaccination’ UK954 outcome is disastrous, but is not a realistic scenario for the reasons stated above, and in the “worst-case” Chart 303 section.
This again emphasises the key role that the UK vaccination programme and similar initiatives in other countries play in our achieving recovery from the pandemic.
In a sense, of course, the very negative impact of relaxed NPIs in the absence of vaccination does underline the importance of both NPIs and vaccination, with NPIs having been the control mechanism available during 2020, and vaccination being the new 2021 option that it is hoped will allow some NPI relaxation, as discussed.
Modelled vs. reported cases and deaths
Finally, I present Chart 209 from the group vaccination model UK957 showing the comparison against reported numbers for cases and deaths overall.

The model does a good job of modelling deaths, but is less accurate for cases. Because live case reporting itself is less accurate, especially early on in the pandemic, I’m not too worried about comparisons with reported cases data, although the comparison is improving, maybe because case reporting itself is improving.
I am more concerned about the 800-day deaths projection. The UK Government, its medical professional and academic advisers, and amateur modellers like me will be looking closely during the gaps between lockdown easing events in April, May and June to reassure ourselves that the rate of easing of lockdown is commensurate with preservation of lives.
Discussion
Further work on data
As can be seen, quite apart from coding development, there is a lot of work in populating models with accurate data, and I have quite a bit to do in this area. I’m pleased with the group functionality and implementation, however, and I think it offers great potential.
Changing age dependency of Covid-19 risks
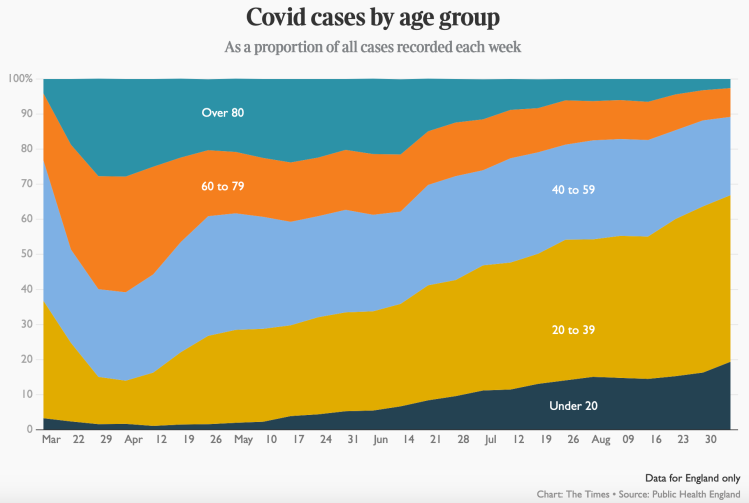
Age has been the single highest differentiator of people’s susceptibility to Covid-19, and I think it’s essential to have an age (and therefore relative risk) dependency structure in the model, so I will persevere with it. This chart from September 5th last year indicates movement in age dependency in case rates, when the disease impact was already beginning to change somewhat, as older people went out less, and younger people worked and socialised relatively more than them.
Today, we see from this slide used in a recent 10 Downing St update that because of vaccination, the relative death rates amongst the age groups is changing:
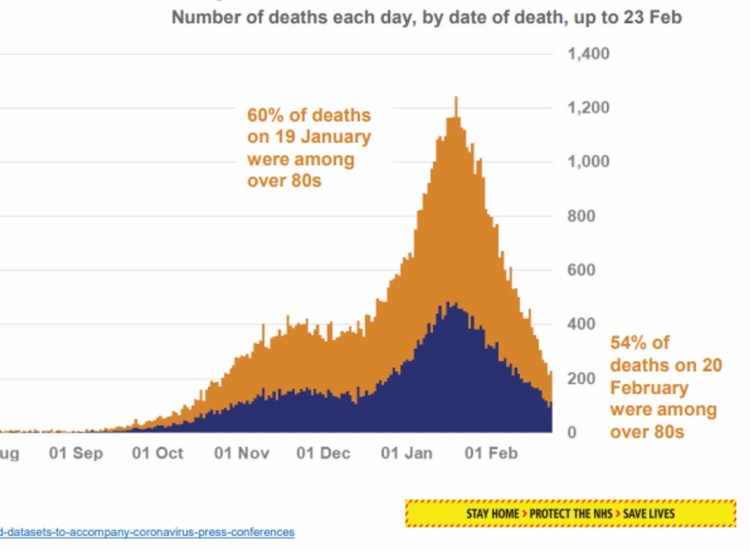
The proportion of deaths which are in the over-80s group is reducing quickly, thanks to the prioritisation of vaccination to those most at risk. There are other risk factors, as for example in this paper which contains the following chart, and these should also be (and are being) taken into account in Government vaccination planning.
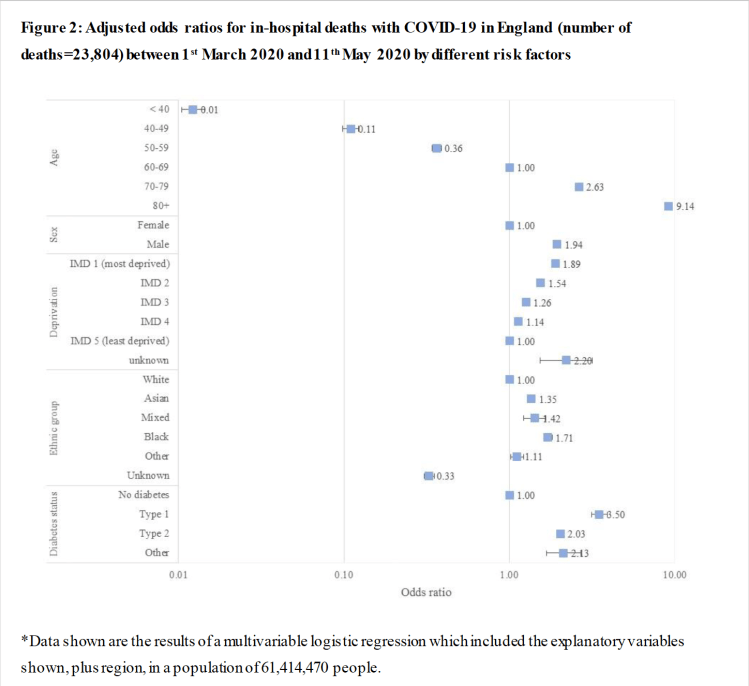
I have referred before to this paper which, while principally driven by the authors’ interest in the risk enhancement of Covid-19 to diabetics, also includes the ratios of other risk factors. The chart showed nearly a 10-fold increase in risk to over 80’s compared with the “control” person in the study; a white female of 60-69 years, with no deprivation or diabetes (ratio of “1” in the chart).
Professor David Spiegelhalter also addressed age-dependency back in May 2020, reported in this YouTube stream, describing the following charts as “startling”, showing as they do a doubling of the risk of death from Covid-19 with every increase of seven years in age at that time. I also covered this session in my May 15th 2020 blog post, where I included all of the slides, including the following one.
The left chart shows the straight line on a log chart which reveals the doubling rate from the slope, and the linear scale chart on the right shows visually the very steeply increasing risk for older people at that time (prior to vaccines), requiring older people prudently to stay indoors more than other parts of the community.

These are the kind of risks that have been changed – improved – considerably by the availability of the vaccines, and prioritised treatment of high risk groups in the population.
Evidence from Scotland for the effect of lockdown and vaccination
These conclusions of the modelling are borne out by the work of Bruce Guthrie, Professor of general practice at Edinburgh University, reported in the The Times on 25th March, who said that the lockdown and vaccines had brought the coronavirus reproduction number down closer to flu levels, and that without these measures the death toll would likely have been much higher.
The reproduction number of coronavirus without any restrictions is thought to be about 3 — meaning every carrier has the potential to infect three others — while flu has a rate of about 1, so flu outbreaks die out quite quickly compared with coronavirus.

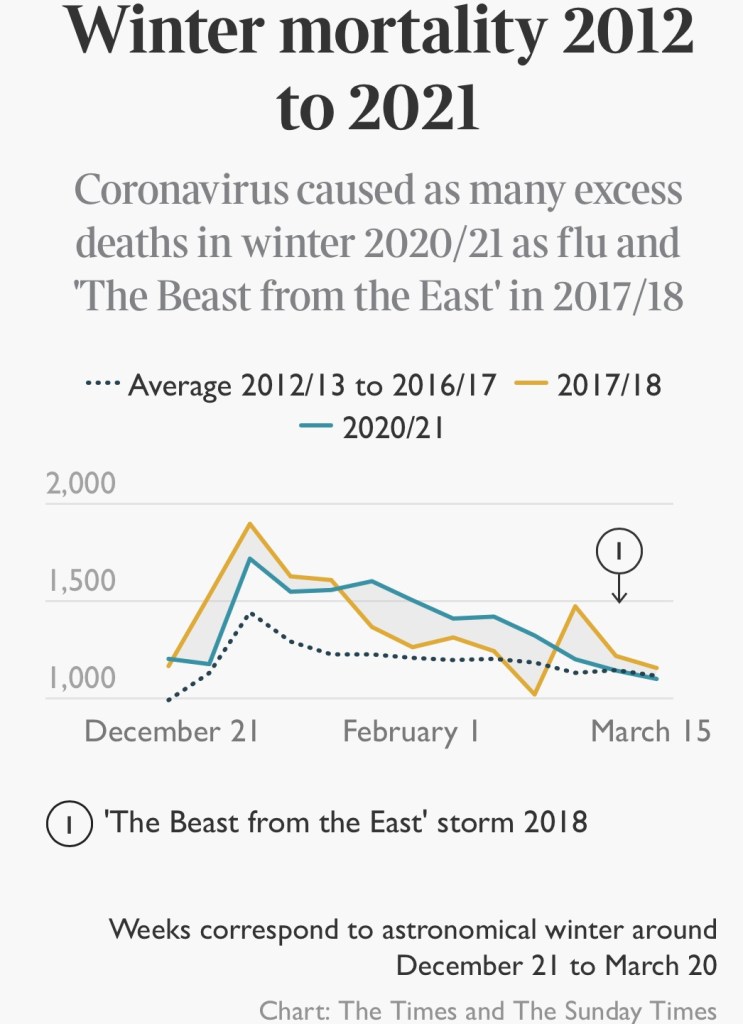
On the right, Winter mortality 2012-2021, and excess deaths flu 2020/21 and “Beast from the East” 2017/18
There were 3,583 deaths in Scotland linked to Covid this winter — including 3,024 where the virus was the underlying cause of death — but no flu deaths and over 1,000 fewer deaths from other respiratory illnesses. There were also over 500 fewer deaths linked to other illnesses that strike primarily in old age, such as cancer and heart disease.
Prof. Guthrie, a member of the UK government’s Scientific Advisory Group for Emergencies (SAGE), said: “We haven’t had any flu this year so if we had no restrictions you would have had a lot of flu deaths alongside Covid deaths. Flu dies out faster as most people have had it before and it evolves relatively slowly, so most people have immunity to whatever strain is spreading each year.
“Flu creates a short-lived spike because it runs out of people to infect, but Covid has created a prolonged death curve since the autumn despite all of the social distancing and lockdown measures.”
Prof. Guthrie said that the vaccine rollout was encouraging but it was too soon to accelerate the exit from lockdown.
The R number for different variants
I covered the relationship between the R number, herd immunity and the disease doubling rate in my blog post on June 28th 2020. Prof Guthrie’s charts indicated that the measures taken to protect against Covid-19 have also protected against flu, leading to little flu mortality this winter. This article by the BBC offers more general information about the R number.
If the transmission rate per day were given by 𝛽 (people per day infected by one infected person) and the duration of that person’s infection is d days, then the number of people infected by that person would be 𝛽d, and so it can be seen in a simple situation that the starting value for R, R0 = 𝛽d. Thus if d were 5 days, say, and 𝛽 = 0.39 as for our first virus variant, then R0 = 0.39×5 = 1.95 for these example figures.
If d were 7 days, R0 = 0.39×7 = 2.73; we see, therefore, that the R number depends on observation of the disease. The corresponding R0 numbers for the second variant with 70% higher transmission 𝛽 = 0.663, for 5 and 7 day disease duration, would be 3.3 and 4.5.
In practice R at any time is calculated from more extended study of the virus and its life-cycle, and depends on the assumed or observed average proximity and mixing of people at any time, and therefore varies over the course of the epidemic (and so it would be denoted R(t) for time t).
Concluding comments and next steps
From the simulation outcomes of the model, it is clear that vaccinations are already making a big difference to the at-risk communities, especially for older and vulnerable people who, from the discussion above, were by far the worst affected by Covid-19 before, and so were the first to be vaccinated.
My next task will be to monitor outcomes as the NPI relaxations take effect, and as more vaccination and hospitalisation data becomes available. I will continue to to check the fSS and fmort variables against current data, for the propensity to serious illness and morbidity, respectively, for different parts of the community from the different variants. It may well be that more disaggregation of the population into groups will be necessary.
I will also be adding functionality to allow the setting of different vaccine efficacy (or a modification of it) by variant, since there is increasing fear that eventually a new variant might appear that is more capable of evading (“escaping”) vaccines.
I haven’t yet added different efficacies to different vaccine types (eg Pfizer modified RNA (mRNA) types vs. the more traditional AZ Oxford weakened virus types) because I handle this in the model at present by setting vaccine introduction dates with different efficacies and daily rates. Obtaining data on who has had, or estimating who will have which vaccine types is probably too difficult anyway.
The overall conclusion, as I said in a recent post, is that the vaccines are the only way of unlocking ourselves from the way of life we have endured during 2020.
And as was suggested in the article I quoted before concerning infectivity of vaccinated people, it’s vital that, even after receiving both doses of the vaccine, that everyone wears masks, practises social distancing and washes their hands when around those who haven’t been vaccinated – just in case.

6 thoughts on “Tuning the age and vulnerability Coronavirus model”