Summary
Having just had my third Covid jab, the “booster” jab, it provoked some thoughts about waning immunity, my Coronavirus model, and the immediate future.
I had incorporated multiple jabs into my UK model some time ago, adding to the capability for multiple phases of rates of inoculation to cope with the rates of first and second jab delivery. I am taking this opportunity to report briefly on model outcomes for waning immunity in the context of booster jabs.
My booster jab
I am in an elderly group, and so, exactly six months after my second jab, I was invited this week to attend for the booster on October 25th. It appeared that all of the others at the vaccination station were of similar – erm – priority (I nearly said antiquity).
Today, in the short queue for my booster jab, I was sitting (socially distanced) next to a 79 year-old man who lost his wife to Covid last year. My own neighbours, both around 40 years young, had long Covid during 2020 and well into 2021. Covid-19 is a very nasty disease. People might forget the scenes from Bergamo back in March 2020. I haven’t.
I chose to have one jab in the left arm (for Covid) and one in the right (for winter flu) so that I could feed back any specific Covid jab reactions to the Zoe app, a UK national Covid-19 monitoring project with over 4m users in the UK, led by Prof Tim Spector.
If I were to have any symptoms from the Covid jab, for example arm pain or tenderness, which are two of the dozen choices in their symptoms menu, I should able to report Covid jab reactions distinctly from reactions to the flu jab. I’m happy to say that only a very slight tenderness is apparent in either arm when palpated, at the moment.
There were no reactions to the first jab all that time ago (2nd February 2021), but I was a little woozy for a day after the second jab (23rd April). As I write this, the day after the third jab (18th October), I have had no reactions at all, just as after the first jab.
I am generally delighted that the Scottish NHS Covid website I use, at https://www.nhsinform.scot, and in particular the part that allows me to monitor my vaccination status at https://www.nhsinform.scot/flu-vaccine/, as advised in the appointment letters, allowed me to rearrange my booster appointment for October 18th (I would have been away on the date that was offered) as well as downloading my vaccination status, complete with Q-codes for each of the first two jabs.
I also like the Scottish NHS vaccination app on my smartphone, which makes me confident, should I need to show information while travelling, that I will be up to date with my vaccination status. All good news so far.
I was in touch with the Scottish NHS support service for vaccinations afterwards, however, wondering why the third Covid jab didn’t appear on my (NHS Scotland) online vaccination record (although the winter flu jab, which I had at the same time, did appear).
I had one or two suggestions, therefore, regarding the vaccination website and the process.
1) Booster jab information on the website (or not)
My phone call to the NHS helpline was made on returning home from my jabs, having checked whether the system had updated my Covid jab status. While it did to some extent, mentioning the third appointment, it only recorded the flu jab, not the Covid jab.
Kelly at the helpline explained that as the third jab isn’t required by third parties yet for any purposes, the website and the app don’t show it.
But confirmation of the winter flu jab isn’t required by any third parties either – but that is recorded there at the website.
That omission is not really sensible in my view. The point of the third jab is to supplement protection in the context of waning immunity, which the earliest evidence I had (judging on the basis of this study in January 2021, https://www.medrxiv.org/content/10.1101/2021.01.13.21249642v1, which had input from all four home nations) indicated that Covid-19 immunity has a half-life of 5 months.
This will depend on whether immunity is from infection or from 1, 2 or 3 jabs, or via a combination of infection and jabs (see the discussion below). In any case, just because those asking for proof haven’t taken this booster jab aspect on board yet, it doesn’t mean that they won’t (and soon if they are sensible). The Scottish NHS system could get ahead of the game by showing the third jab status for people who have had it.
2) Website design
Logging into the website is fine if you have the link that is printed in the vaccination invitation letter, www.nhsinform.scot/flu, which I do, but if you just go to www.nhsinform.scot, as I did when my letter wasn’t to hand, using a different browser (and device) so that it wasn’t in my browser history, it is VERY hard to find the link to login. You have to go, as was explained, to a second page, and then scroll down a long way to pick up some hypertext about finding vaccination status.
These days, the vaccination status is something that a lot of people will be wanting to access, and I think it should be boldly present on the opening page of www.nhsinform.scot, and not buried far down on a subsidiary page.
3) The need to see all jab information
The need to see that third jab status isn’t so academic in the UK either. Some people who have had two Astra-Zeneca (AZ) jabs might have had one of them from the AZ batch that wasn’t, and may still not be, recognised in Europe. That batch comprised 6 million of the AZ doses that were made in India, whose manufacturer hadn’t yet applied for certification in the EU. The compound is exactly the same as those made in the UK, but it needs to be separately certified in the EU.
I had hoped that when such recipients got their booster (third) jab, which wouldn’t be from that batch, they would be able to show two jabs that ARE acceptable (the first and the third, say) for travel to the EU. But they can’t if it isn’t on the app or the website.
The Scottish NHS helpline took all this on board, and as I indicated that a) I have been a web designer in the past during a long career in IT, and b) because I model and take a keen interest in the pandemic, they asked me to put it all in writing. I did so, and I have summarised it here too.
Model capabilities
My model copes with all NPIs (Government mitigations); vaccines, in multiple phases of rates of delivery (up to 1/2 million or so per day at times); multiple variants (3 at the moment – original, Alpha and Delta); multiple jabs (up to 3 so far); multiple population groups (4 at the moment); immunity waning; vaccinated infectivity (because vaccinated people CAN transmit the disease); vaccinated illness (vaccines aren’t quite 100% efficacious) and deaths (there is SOME breakthrough resulting in deaths); vaccine hesitation, and a lot more besides. I have been focusing on this (as an individual) for a long time.
Vaccination, community (herd) immunity, and immunity waning
You will have seen in my blog that I have been saying since mid-2020 that a vaccine programme was, and is the only way through this crisis. Herd immunity (discredited as a primary starting approach, but something that will need to be achieved) can only reach the required 80%+ of the population through vaccination.
The Delta variant has reinforced that position. The Herd Immunity requirement H% is given by
H% = (1 – 1/R0)x100%,
where R0 is the reproduction number, equivalent to the number of people one person might infect in a well-mixed population. For Delta, whose R0 is around 7, this would mean that H needs to be 85% or more. Alternatively, as I showed in my June 28th 2020 blog post, H can also be calculated from the case doubling time TD and the disease duration d, which can sometimes more easily be observed from the regularly published timeline of data:
H% = (1-TD/d(loge2))x100%,
because as I showed in my technical paper in April 2020, R0, TD and d are related by
R0=d(loge2)/TD.
When vaccine hesitation is taken into account (which varies between age groups (in the model too) and also because not all parts of the UK population have been offered the vaccine yet, this will be a tough target to reach. You can see more about how H is calculated in my 28th June 2020 blog post.
As I write this, I am disappointed to see that over 5 million eligible people in the UK over the age of 16 remain unvaccinated. On a more positive note, over 4 million have had the booster, out of 8 million eligible so far (on the basis of the 6 months interval since their second jab), although that seems to offer considerable scope for improvement too.
Most reports I have seen indicate (for example this one about the Swedish experience, that I reported in my August 14th 2020 blog post) that only 20% community immunity to Covid-19 is reachable though natural infection, and for a nasty and dangerously fatal disease like Covid-19, that simply isn’t ethical (or feasible) given that many deaths would ensue, even more than we have suffered on our path through 2020-21.
The study about waning immunity I spoke about, https://www.medrxiv.org/content/10.1101/2021.01.13.21249642v1, which has input from all four home countries of the UK, is referenced in my blog post at https://brianrsutton.com/2021/03/26/age-and-vulnerability-related-coronavirus-modelling/ back in March this year.
Two comparative model runs for different immunity waning settings
This led me some time ago to introduce immunity waning to the model, and I have made one or two parametric runs (in the new booster jab context) with different settings. One, UK076, has immunity waning half-life set to 75 days for all situations: infected with no vaccination, and for 1, 2 or 3 jabs, whether infected or not.
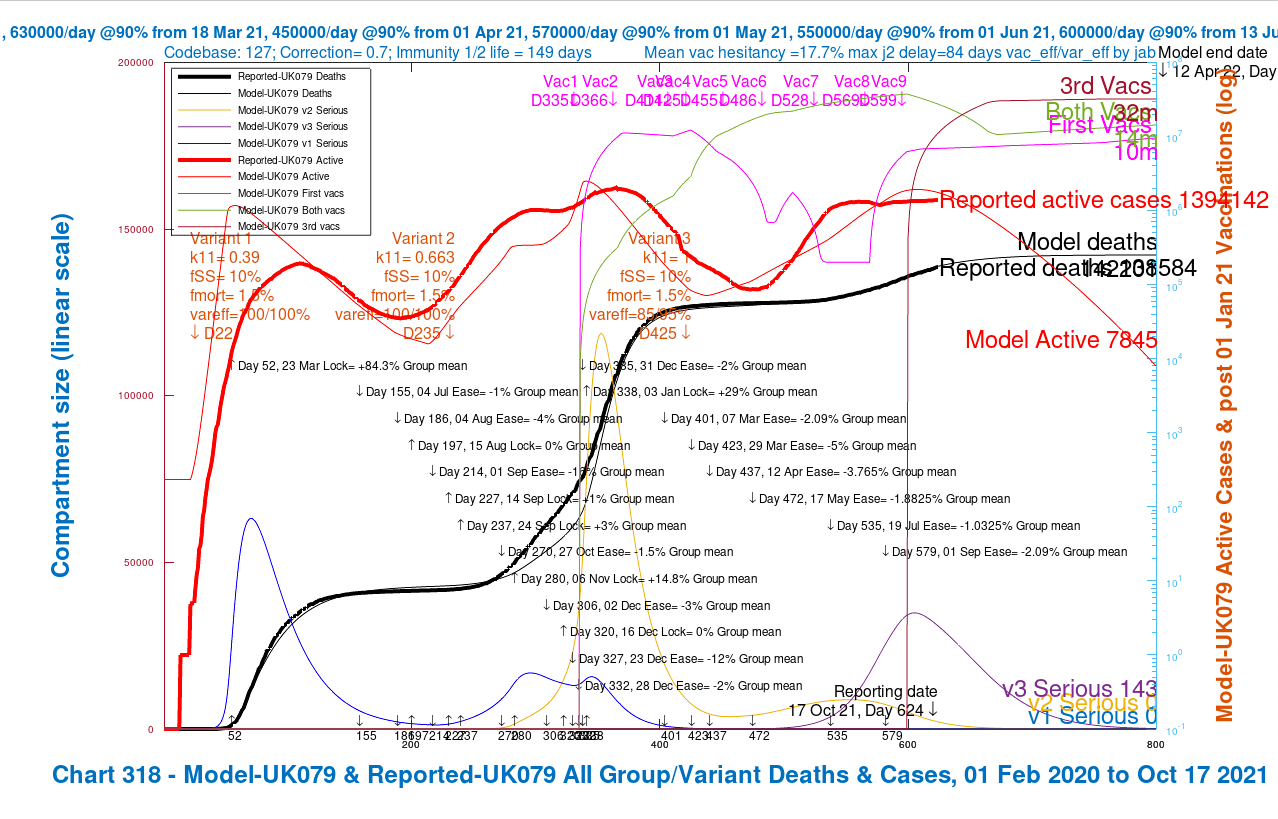
UK079 was run with the immunity waning half-life set to a more realistic 150 days for all population groups and their jab situations – none, 1, 2 or 3.

In these charts, you see that the projected deaths for scenario UK076 at 164,091 for “fast” immunity waning, at 75 days half-life, is far higher than for my scenario UK079 “standard” immunity waning half-life of 150 days, at 142,201 deaths, showing that immunity waning can make a big difference to pandemic outcomes.
The active cases, you will notice, peak in my model for both scenarios not long after the current reporting date, 17th October (624 days into the model from the outset of the pandemic).
Thereafter, the model has no further Non-Pharmaceutical Interventions, (NPIs) or changes in public behaviour (informal relaxation of precautions), beyond the most recent change when schools returned on 1st September.
But last year, running the model both for the USA at Thanksgiving, and also looking forward to the UK Festive and New Year period, there were large fluctuations in the cases (and deaths). This year, I would expect an increase in active cases, but less so in terms of serious illness and deaths, thanks to the vaccination programme. I’ll be modelling the end of year period soon.
Immunity waning discussion
The charts above beg a question: what are the real half-lives in different situations? Natural immunity – bestowed by having been infected by Covid-19 – and immunity offered by vaccine jabs might be expected to be different in extent and duration. One study, at least, found such differences.
This non-peer-reviewed article from August 2021 from authors based in Israel, a country that was very early into a vaccination programme, concluded “This study demonstrated that natural immunity confers longer lasting and stronger protection against infection, symptomatic disease and hospitalization caused by the Delta variant of SARS-CoV-2, compared to the BNT162b2 two-dose vaccine-induced immunity. Individuals who were both previously infected with SARS-CoV-2 and given a single dose of the vaccine gained additional protection against the Delta variant.“
I have therefore added another comparison, run a couple of days later, where I leave immunity waning at 150 days for unvaccinated (but infected) people, but set it lower, at 75 days, 100 days and 125 days for 1, 2 and 3 vaccination jabs respectively, bearing in mind the Israel study referenced above.

Chart 318 for scenario UK079 with vaccinations. 17th May 1.8% ,19th July 1% and 1st Sep 2% mean NPI relaxations. v3 transmission k11 = 1, var_eff = 85/95%, fss x1 and fmort x1. Model 800 day outcomes to April 12th 2022 compared with reported active cases and deaths to October 17th. Serious cases for 3 variants 
Chart 318 for scenario UK067 with vaccinations. 17th May 1.8% ,19th July 1% and 1st Sep 2% mean NPI relaxations. v3 transmission k11 = 1, var_eff = 70/85%, fss x1 and fmort x1. Model 800 day outcomes to April 12th 2022 compared with reported active cases and deaths to October 19th. Serious cases for 3 variants
The simple (unweighted by population numbers) average waning half-life is lower, at 104 days, in Scenario UK067, where it remains at 150 days for unvaccinated people, with a sliding scale of 75, 100 and 125 days half-life for 1, 2 and 3 jabs respectively. The outcomes, however, are very similar to the 150-day UK079 “base-case” version.
The small differences are also dependent on the higher vaccine effectiveness to Variant v3 (the Delta variant) in UK067 than in the base case UK079, although still as high as 85% and 95% for single and double jab efficacy compared with the first two variants. The peak in active cases in UK067 is a little higher, but projected deaths are much closer than the previous comparison, now at 142,584 compared with 142,201 in the UK079 base-case.
The closer outcome for projected deaths is because the immunity waning for infected (but unvaccinated) people applies to all infected people throughout 2020, as well as in 2021, which leads to growth in cases and deaths from very early on in the earlier Scenario UK076 which had the short, 75-day immunity waning half-life for everyone infected.
Any differences in immunity waning for vaccinated people, conversely, apply only to 2021, since vaccination became effective only at the turn of the year, starting with the first patients few patients on December 8th 2020.
We see here some of the complexity of the data dependencies of the model (and the pandemic) to many overlapping factors determining the rate of growth/decline of the prevalence of Covid-19 infection.
Further published studies on immunity waning
Another study, just reported in Nature, using estimates based on viral evolution, forecasts a 50% risk of re-infection 17 months after a first infection, without measures such as masking and vaccination. Sarah Cobey, an evolutionary biologist at the University of Chicago in Illinois, underscores the need for people who have been infected to bolster their protection with a vaccine — a point driven home by research published by the US Centers for Disease Control and Prevention in August.
The study looked at people infected by COVID-19 in 2020, some of whom became reinfected in May or June 2021. It found that those who had not had a vaccine were more than twice as likely to get reinfected in that period as those who had both the virus and a vaccine3. That Nature article was looking at the related concepts of COVID hybrid- and super-immunity, and is also worth reading. See all the references below.
The Zoe project that I mentioned before has also published a good review of the evidence it has seen on natural and vaccinated immunity here.
What might happen next?
With booster vaccinations now being offered, there are quite a few combinations of infections vs. vaccinations to be implemented in models like mine, delivering differing degrees/durations of Covid-19 immunity depending on the number of vaccinations (including none) and whether a booster jab has been taken. As we saw above, the half-life of immunity waning, including to which parts of the population it applies, and by how much, can make a large difference to outcomes.
My expectation, therefore, is that to keep our immunity up to date as Covid-19 becomes endemic in the UK, we will be taking annual, or more frequent, perhaps bi-annual inoculations as a matter of routine, just we do for winter flu.
The coming winter will also tell us something about influenza in the Covid-19 context. Last winter, in the UK, the incidence of winter flu in the UK was much reduced, possibly because of the many behavioural precautions we were taking habitually because of Covid-19. Some expect this winter to be far worse than usual for winter flu, given the lack of natural immunity from last year (even if it lasts that long), and depending on which strains of influenza we have this year. We will see.
The vaccination programme remains vital to controlling the pandemic. Vaccine hesitancy, any diminution in vaccine efficacy to a possible new variant, perhaps, or major relaxations in public caution will change the situation. The UK Government list of variants, and their rates of occurrence shows many Variants of Concern (VoCs) or under Investigation (VuIs).
The AY.4.2 sub-variant
A new sub-variant (of Delta), designated AY.4.2, was mentioned in the Government briefing today, and appeared in the October 15th Government Technical Briefing document, in the Epsilon section, in “monitoring” status. We already see tangible growth of its presence, just as I remember we did early on with the Alpha and Delta variants.
Update: The AY.4.2 sub-variant is now known as VUI-21OCT-01, now being under investigation, and appears as such in the newly published October 22nd Government Technical Briefing Document under the Delta lineage.
In their October 18th Financial Times report “New Delta descendant may be more infectious than its ancestor“, Clive Cookson and John Burn-Murdoch (excellent sources for good analysis of the pandemic) said “Scientists say AY.4.2 seems to be 10%-15% more transmissible but cannot be blamed for high UK Covid-19 case numbers“.

I suspect they feel that AY.4.2 “is unlikely to be the game-changer that Alpha and Delta were” because it has arrived when the vaccination status of the population is high (although should be higher). My previous modelling, for example here in January 2021, has indicated that postulated variants that arrive into an environment of high NPIs – Non-Pharmaceutical Interventions, such as social distancing, mask wearing and working from home – tend to die out more quickly.
My subsequent blog post on 12th February indicated how increasing rates of vaccination allow us to reduce NPIs, controlling the growth of Covid-19 infections through pharmacological methods rather than with NPIs only. This partial “equivalence” of the effect of NPIs and vaccination on current infection rates indicates that the faster damping down of the growth of a new variant would also apply in a context of high vaccination levels.
Comparative parametric runs of my model reported in my blog post on 14th April confirmed that a new variant with high transmission, introduced when there is no vaccination, grows very rapidly, but can be controlled with vaccination. The great advantage of vaccination over NPIs, of course, is that the benefits endure (subject to booster vaccinations as described above), allowing us increasingly to lead more normal lives.
Prof. Francois Balloux, of University College, London, also felt that AY.4.2’s small increment of 10/15% in transmission rate compared with Delta would not have a comparable impact on the pandemic. He said that Denmark, who, just like the UK, detect new variants quickly because of their excellent genomic sequencing, had seen AY.4.2 reach 2% frequency, but that it had died down since.
I expect to be adding changes to my model data to reflect more relaxed public behaviour in the lead-up to the Festive period and New Year, possible paralleled by changes to Government recommendations regarding the NPIs we have all come to know so well.
I will also consider whether I should add this new variant to the model, although as we have heard, others don’t expect it to have a major impact. My model, as outlined above, also offers hope that AY.4.2’s effect will be limited, as long as we can maintain, and even increase vaccination rates.
What Government and the public can do – concluding thoughts
The UK Government’s Plan B – including masks, working from home and vaccine passports – has already been outlined by Government to prepare us for such eventualities. A Plan C, which could include a pause of household mixing, is rumoured to be under discussion by Government.
Meanwhile, the current programme of booster vaccinations should save us from the worst outcomes of immunity waning. A Pfizer study reportedly shows that it will add higher levels of protection too. Some in the UK are dissatisfied, however, by the rate of delivery of booster jabs. It is certainly vital that they are given very soon after 6 months after the recipients’ second jabs, given a presumed 5-month half-life of immunity.
In England, people may now book their booster vaccination online in the week after the six-month point. I hope that this will extend to the Scottish NHS, since I am aware that some who qualify in Scotland have not yet received their booster (or winter flu jab) invitations.
I continue to wear a mask in indoor public places and on public transport, on the rare occasions I am in those situations, minimising travel as I do.
Why? Because it not only protects me, to some extent, but also others. A fully vaccinated person, even if not infected themselves, can still carry the infection, and can spread it from their airways, as reported by Nature in August 2021, on the basis of several studies I have referenced below.
The viral load carried by a vaccinated person was found to be lower, however, meaning that vaccinated people should be less infective, and for a shorter time than unvaccinated people. But it is clear that mask wearing, even by those fully vaccinated, helps protect others.
Also see point 20 from the 9th September UK SAGE Committee report which states “SAGE noted that European comparators with similar levels of vaccination have maintained more interventions (masks, vaccine certification, work from home) than the UK and are seeing their epidemics decline.”
As Kenneth Wolstenholme didn’t quite say: “They think it’s all over; it isn’t yet”.
References for immunity waning
- Townsend, J. P. et al. Lancet Microbe https://doi.org/10.1016/S2666-5247(21)00219-6 (2021). PubMed Article Google Scholar
- Edridge, A. W. D. et al. Nature Med. 26, 1691–1693 (2020). PubMed Article Google Scholar
- Cavanaugh, A. M., Spicer, K. B., Thoroughman, D., Glick, C. & Winter, K. Morb. Mortal. Wkly Rep. 70, 1081–1083 (2021). PubMed Article Google Scholar
References for vaccinated infectivity
- Riemersma, K. K. et al. Preprint at medRxiv https://doi.org/10.1101/2021.07.31.21261387 (2021).
- Brown, C. M. et al. MMWR Morb. Mortal. Wkly. Rep. 70 1059–1062 (2021).PubMed Article Google Scholar
- Musser, J. M. et al. Preprint at medRxiv https://doi.org/10.1101/2021.07.19.21260808 (2021).
- Chia, P. Y. et al. Preprint at medRxiv https://doi.org/10.1101/2021.07.28.21261295 (2021).

3 thoughts on “Coronavirus booster jab matters”