Introduction
*Winston Churchill once described the successful end of the second battle of El Alamein (the defeat of Rommel) as the “end of the beginning“, rather than as the beginning of the end of the 2nd World War.
I feel that way about the announcement today, December 2nd, that the UK’s MHRA (the UK’s Medicines and Healthcare products Regulatory Agency) has approved the Pfizer/BioNTech vaccine for release in the UK, reportedly intended for distribution the following week by the UK Government.
At the same time as the UK Government has introduced more stringent Covid-19 Tier arrangements in England (with parallel and slightly different measures in each of the other UK home nations), some relaxation of the measures has been announced for the 5 days of the festive season (allowing an extra day (6 in all) for those travelling to and from Northern Ireland).
As I reported in my most recent blog post on November 25th, and as we have also heard in Downing Street briefings, scientists are expecting that even with a vaccine, we will be feeling the impact of the winter period, in terms of a possible further phase of the epidemic, until March at least. The festive season relaxations, while welcome, are bound to mitigate the effect of current interventions to control the virus.
Thus, just as Churchill’s announcement was made in 1942, during a war that went on until 1945 (even the Normandy landings weren’t until mid-1944, leading to the end of the war in Europe), this vaccine approval announcement is welcome, but isn’t necessarily the end phase of the epidemic even in the UK, let alone world-wide. Rather, it marks the end of a significant period of uncertainty, and the start of justified evidence-based hope, bordering on expectation.
Now that it seems, therefore, that a vaccination programme in the UK might start as early as next week (for the first doses, given to the priority parts of the community), I have re-run my Covid-19 vaccination model for the UK, updating my November 25th scenarios to reflect some potential UK outcomes.
The UK announcement
Today’s MHRA announcement was led by their CEO, Dr June Raine, supported by Prof Sir Munir Pirmohamed, of the University of Liverpool, Chair of the Commission on Human Medicines (CHM) Expert group, and by Wei Chen Lim, Professor of Respiratory Medicine at the University of Nottingham, and representing the JCVI, the Joint Committee on Vaccination and Immunisation, who advise the UK Government on priorities.
The following slides were shown at the presentation. They show, as I indicated before, that both the development and the approval processes have been run in parallel to shorten the whole process leading up to the release of the vaccine. They also confirm, much as expected, the priority groups for the vaccine roll-out, led mostly by the significant age related risk groups for Covid-19, and also taking into account other ethnicity, deprivation and access to healthcare dependencies.
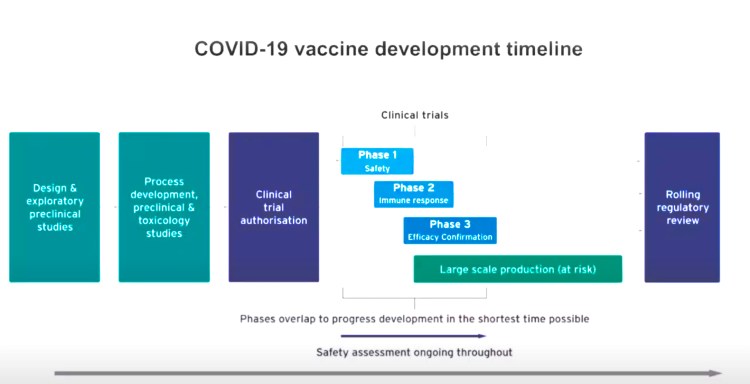
How the development life-cycle for a vaccine has been shortened 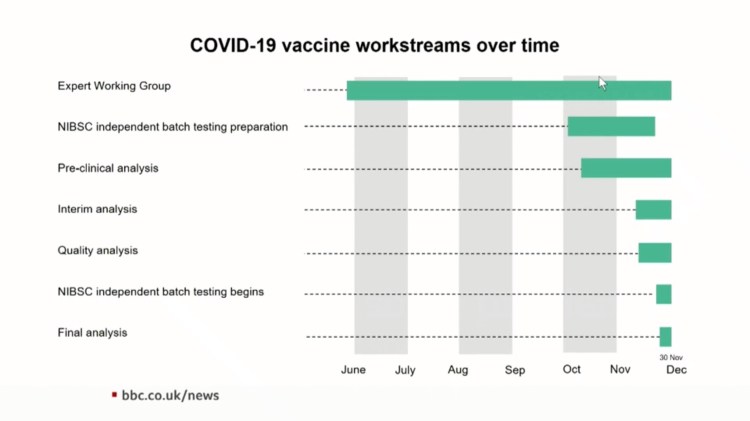
How the approval life-cycle for a vaccine has been shortened n the UK 
The process of assessment of the safety and priorities for the UK vaccination offer 
The principles assessment of the first-phase vaccine prioritisation 
Priority groups for vaccination offer, confirmed in the December 2nd announcement 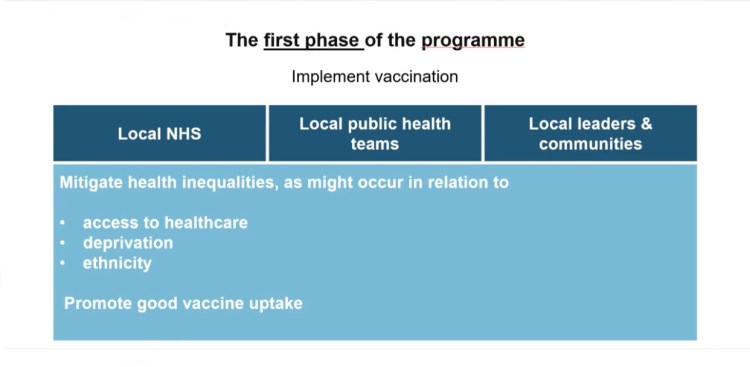
First phase of the UK vaccine distribution programme
This presentation was followed by a Downing St presentation later in the day, during which this key point was made:
Because protection from the vaccine is only conferred properly after the second, booster vaccination, even for priority groups who get their first inoculation in early December, protection will not start until the early New Year, once they have had their second inoculation 3 weeks after the first one, and then only after another 7 days. So it’s a month before the first people will have protection from Covid-19.
Thus my judgement last time to run my model from a first vaccination date of January 1st 2021 was probably about right (in terms of when the vaccine might begin to protect people).
I had been pessimistic, however, in setting the efficacy of that first month of the inoculation programme at 70%. As this Pfizer/BioNTech vaccine is said to have an efficacy of 95%, I will therefore adjust that setting in my model throughout the modelled vaccination programme.
Model outcomes for the postulated vaccine programme
Another variable in the process of a vaccination programme is, of course, the pace at which people can be inoculated. I had set that at 100,000 per day for the first month, and then 200,000 per day for 6 weeks, followed by 300,000 per day thereafter.
I have been monitoring announcements carefully, and I will set the same roll-out profile for now, and adjust when I can be more certain. I hope/expect that eventually the 500,000 per day target might be achieved (1500 inoculation centres working at an average of 350 inoculations per day as stated in my November 25th post).
450 day outlook (to April 27th 2021)
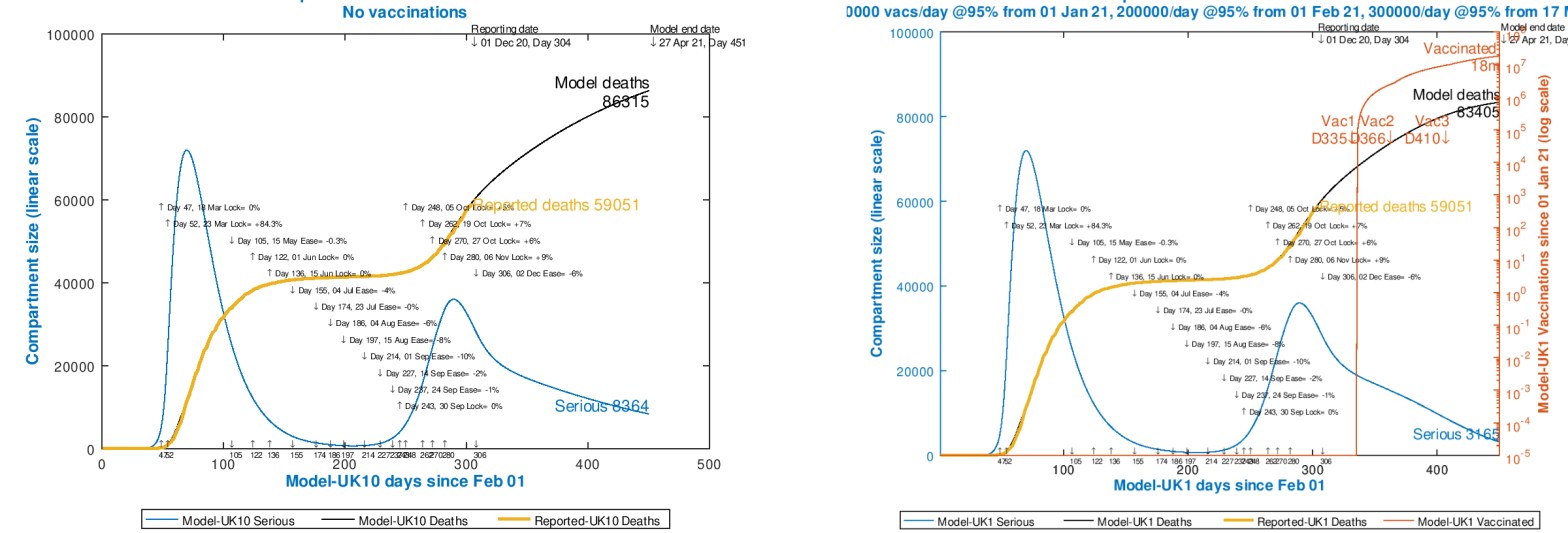
First, then, for comparison purposes, a comparison of the “no-vaccination” case, the same as before, for 450 days (to April 27th 2021), with the vaccination case. Drag the slider up and down to see the comparison between the two cases. I have assumed the same Non Pharmaceutical Intervention (NPI) programme for each, and for consistency and comparison with my previous forecasts.
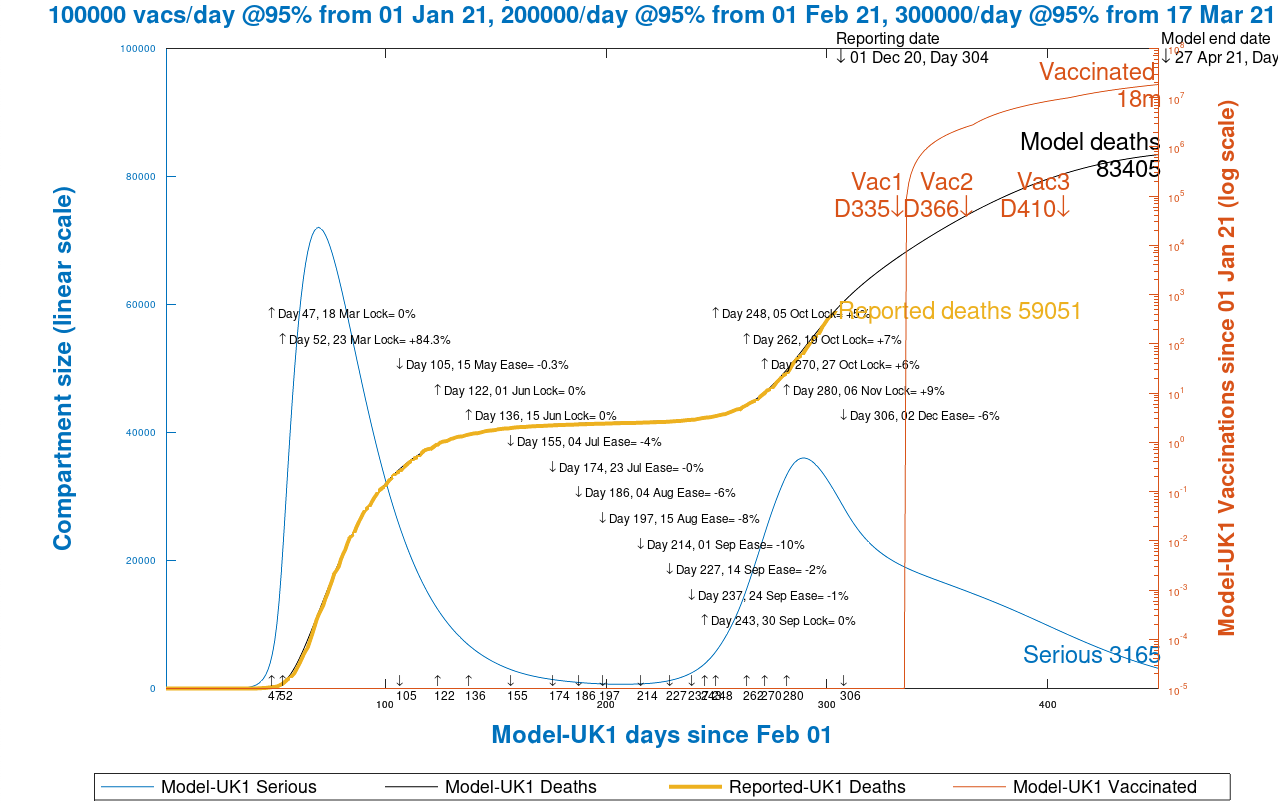
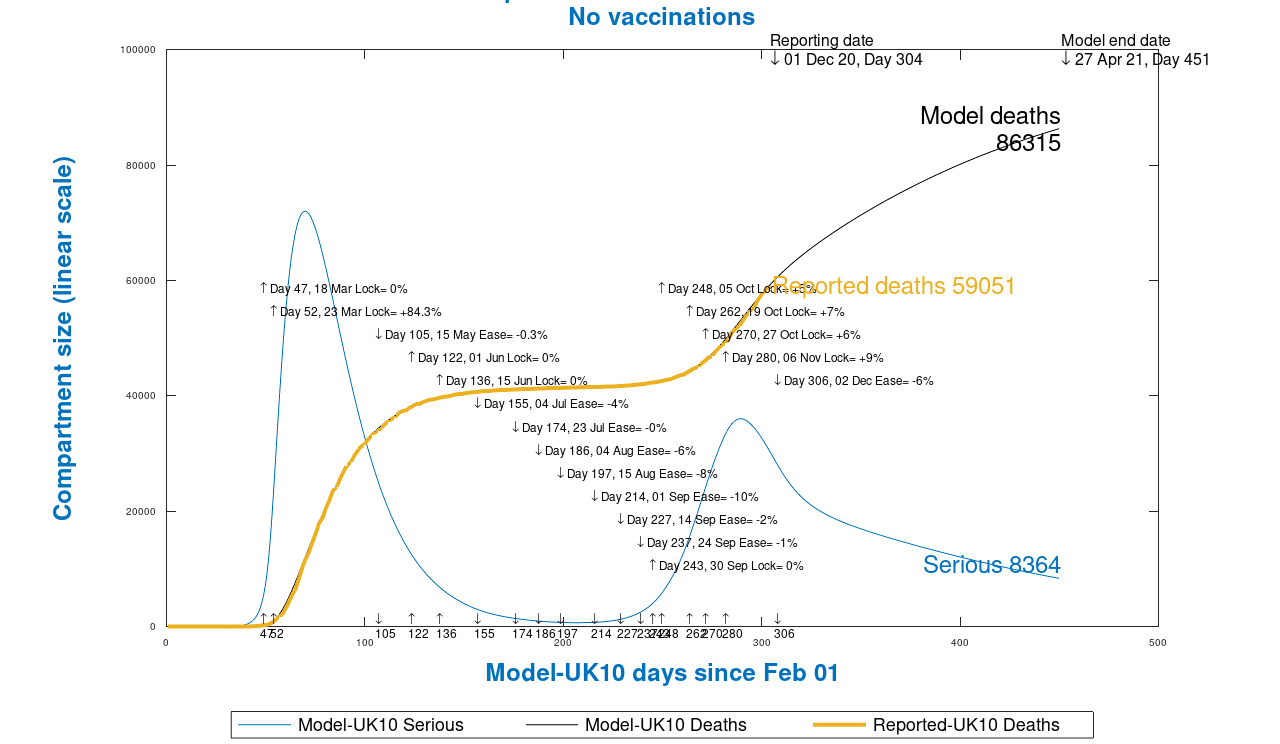
We see that there are 86,315 forecast deaths without vaccination and 83,405 with the vaccination, saving 2,910 lives by April 27th next year. According to the modelled vaccination schedule, 18 million people have been vaccinated by that date.
800 day outlook (April 12th 2022)
450 days of model time is quite a short time (only 115 days of vaccination effect from January 1st 2021), and so I also look out to 800 days – April 12th 2022 – to see a longer term comparison. Again, drag the slider up and down to see the comparison.


Here we see that for the longer term, 800-day model outlook, there would be 98,080 deaths without vaccination, and 84,461 with the vaccination programme, saving 13,619 lives. According to the modelled vaccination schedule, 53 million people are vaccinated by April 12th 2022.
Of course, in that extra year there would no doubt have been other NPIs (Non Pharmaceutical Interventions) in the absence of (or even with) the vaccine, but it does show the full effect of what the vaccine can achieve, given time to take cumulative effect.
Discussion
The need for a vaccine
Just as for today’s announcement, this model comparison is just a first step in assessing possible outcomes in a vaccine context. There is no doubt that a vaccine is needed, and I have rehearsed the arguments (most recently in my November 25th post) about a vaccine being the only way to achieve community immunity (“herd immunity”) practicably, safely and/or ethically; such immunity is not reachable through natural infection.
The effect of the vaccine in the 450 and 800 day cases might seem low, however, in terms of saved lives.
To show the high potential impact a vaccine can have on saved lives, I have run the model as if a vaccine were available, which of course it wasn’t, at the initiation of the model (February 1st 2020) for the UK, which calibrates the possible effect a vaccine can achieve over a long period.

I showed a similar result in my post on November 18th, but with a lower efficacy, and this outcome is consistent with that, with more lives saved by starting with 95% efficacy immediately, as well as with the increasing inoculation profile as in the previous cases above. In other respects the conditions are the same, with other NPIs the same as then, and as above.
Even at a vaccination profile per day of 100,000 rising to 300,000 (still much less than the UK Government hopes for), the previously modelled 98080 deaths for 12th April 2022 (Day 800) are significantly reduced to 15,262, an outcome that Sir Patrick Vallance (the UK Chief Scientific Adviser) said, all that time ago in late March, at less then 20,000 would be a good result (a hope rapidly overtaken by events).
A major positive effect of the vaccine, at this stage, is that Non Pharmaceutical Interventions (NPIs), all part of the partial lockdowns we have become used to, can be reduced, and eventually removed, with consequential positive benefit to our mental health, social engagement, wider societal health and the economy.
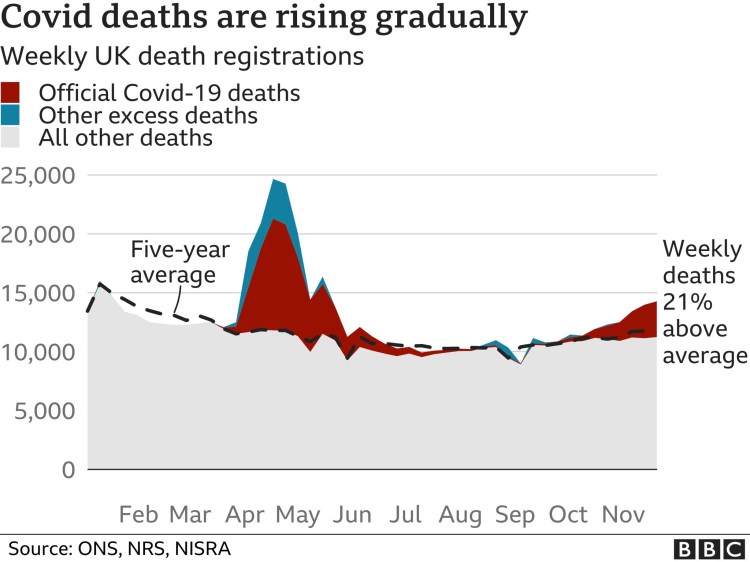
Excess deaths
I also emphasised in my November 25th post (as before) that those who appeal to the “excess deaths” measure as indicating that Covid-19 is not much worse than seasonal influenza are wrong. Even if excess deaths had reached zero (which they haven’t, sustainably – see below), Covid-19 deaths have already more than replaced lower rates of deaths arising from previously normal travel and work patterns.
Covid-19 has also caused longer term illnesses (“long-Covid”); the self-isolation, social distancing and quarantining necessary to control it (which are the reasons why, without a vaccine, it has been able to be controlled to any extent at all) do and will result in more deaths and illness from depression and from dread diseases, which won’t have been diagnosed to a sufficient extent, or early enough this year. A King’s College London study states that we are storing up many deaths for the following years, and there are other reports of such likely increases from similarly well-qualified sources.
As I have said before, deaths from Covid-19 are not the only measure of human suffering from the disease.
As for the excess deaths count – it’s on the rise, just as we know that Covid-19 cases and deaths are on the rise.
Vaccine options
There is a long list of potential vaccines, and after today’s announcement of the Pfizer/BioNTech UK approval, the Oxford/AZ and Moderna ones will probably be the next to be approved.

As I mentioned in my November 25th post, the different vaccines are based on different technologies, with different costs and characteristics, and the leading ones are summarised as follows.

These differences – such as between the RNA and Viral vector ones – are the subject of study relating to their relative propensities to generate active T-cells (key to immunity duration), and whether the vaccines might be safe for those with compromised immunity, whether through disease or from therapies to treat other diseases. Answers so far seem reassuring, but please check if you need to know for sure.
In my most recent blog post, I provided this link to the “Ask the Experts”: YouTube video from November 25th about vaccines in the Covid-19 context. It is must-watch video for anyone interested in Covid-19 vaccination (all of us?) with Prof Tim Spector, professor of genetic epidemiology at King’s College London and the Zoe project, and Prof Peter Openshaw of Imperial College, hosted by Christina Hu of the Zoe Covid Symptom Study, and these vaccine differences, and a lot more were covered in that session.
The UK’s relative position
In this post, I have presented projections only for the UK, as the USA has not yet approved any vaccine (in common with all other countries apart from the UK, so far). The mix of potential vaccines opportunities vary with the pre-purchasing situation in each country, of which I show several below, from Nature Magazine, from which we see that the UK is relatively well placed.

Within the UK, as we saw from the MHRA presentation slides, there will be a priority order for the dispensing of the vaccine to different vulnerability groups. Here is a little more on that topic, including the relative size of the groups, summarising Government advice on the priorities for those groups, from the ONS (UK Office for National Statistics) and others.

Worldometers comparative projections for April 1st 2021
I note that the University of Washington forecasting page for the UK is now showing a variation for rapid vaccination, and I thought I should present that alongside my projections for comparison, although assumptions will be somewhat different.
The University of Washington UK forecast to April 1st 2021 (which is Day 425 in my model), with data drawn from current data at the Worldometers UK web page, shows the following projection for April 1st 2021:

As we see, their projection for universal mask wearing seems independent of the projection for rapid vaccine rollout, whereas my vaccination model forecasts include both dispensing of vaccine, according to the schedule I have used above, and also all NPIs – mask wearing, and other social distancing according to UK Government requirements and/or advice.
My model’s intervention status would probably be greater than that for the University of Washington model outlook. My model’s two forecasts, one for no vaccinations, and one for my usual vaccination schedule, to April 1st 2021, are as follows, with all interventions tabulated in the charts.
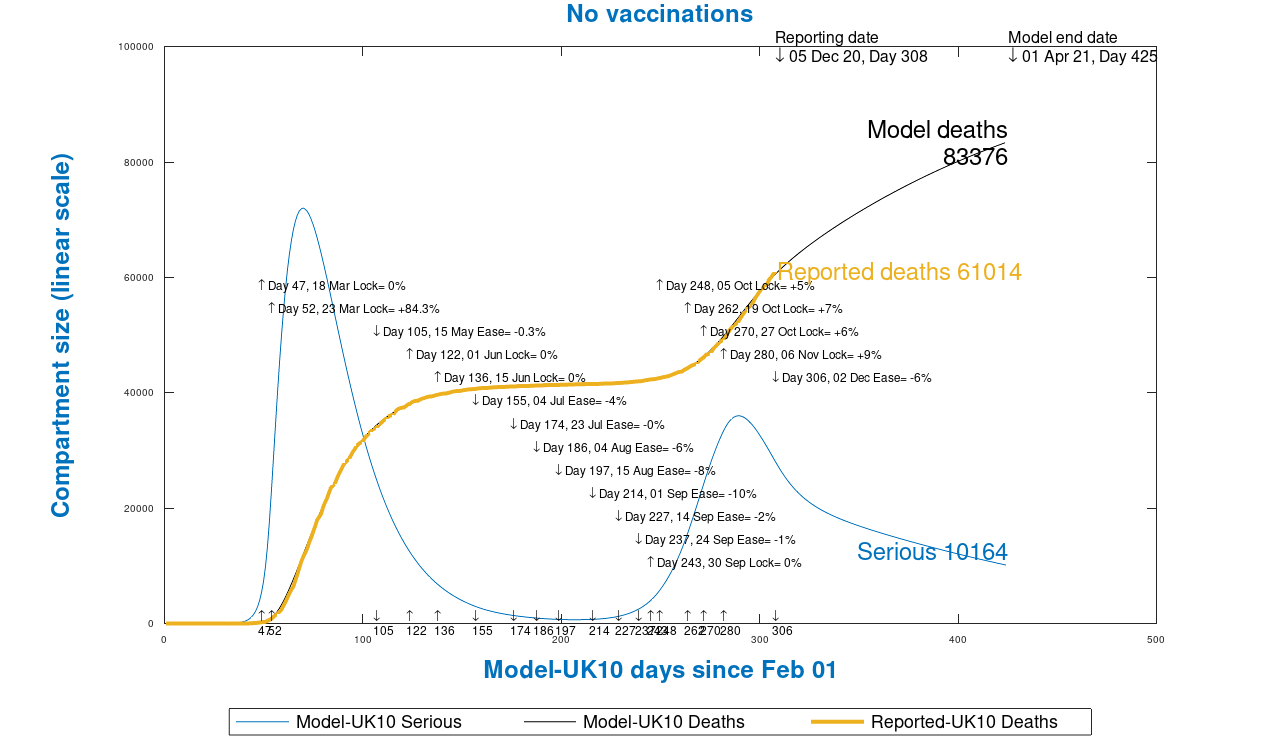
My forecasts seem to be more optimistic, and we can see some differences in assumptions, both in vaccination efficacy and in festive season interventions in the relevant University of Washington forecasting policies document for the UK. In any case I present these comparisons for completeness.
We have yet to navigate the festive season, and the relaxation of interventions might well make a difference, as Thanksgiving in the USA has done recently, with quite an increase in the daily rate of USA cases and deaths. That should be a lesson to the UK, and I will look at this in my next post.
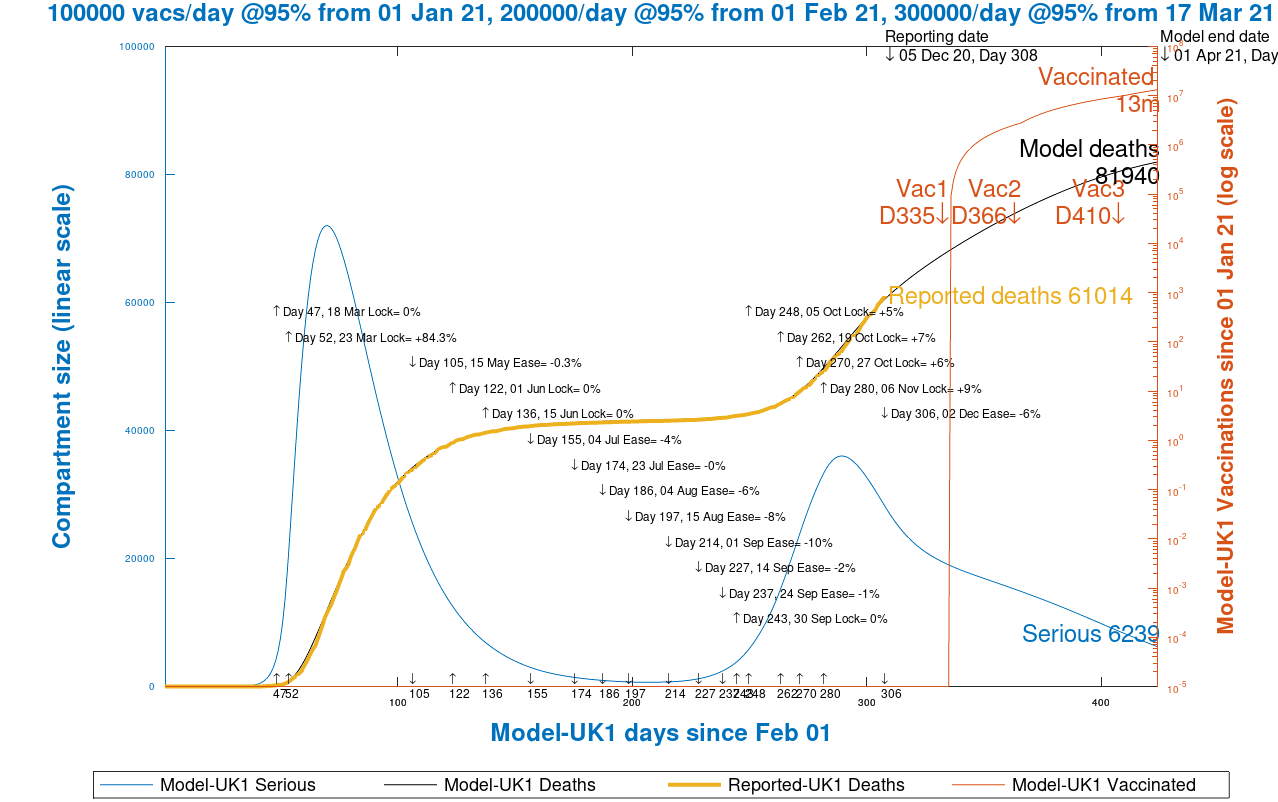
The limited impact of just a 3 month ramp-up of the vaccine can be seen; 83,376 minus 81,940 = 1,436 lives are saved during the 3 months of vaccinations in January, February and March, totalling 13 million vaccinations in the model, although, as I said, those receiving it will increasingly feel safety, security and freedom in their lives as more of the population is inoculated.
Concluding thoughts
This has been exciting news for the UK today; it was very open of Professor Jonathan Van-Tam (UK Deputy Chief Medical Officer) to express his emotional state when he heard the news this morning. Although we are a long way down the track with millions of cases and tens of thousands of deaths in the UK, we can now have hope, and even expectation that we have a route out of the epidemic.
All involved have stressed the need for people to take the vaccine. Clearly we will face the issue of what Professor Calum Semple, Professor of Child Health and Outbreak Medicine, Consultant Respiratory Paediatrician at Alder Hey Children’s Hospital, earlier in the day, called, with admirable honesty and directness, “the lunatic fringe”, who tell us that the vaccine contains microchips to control us, and/or a range of other crazy antivaxxer fear-mongering, pseudo-scientific claptrap.
But to end on a justifiably positive note, Covid-19 may well become endemic, just like seasonal influenza (even though, without a vaccine, Covid-19 is far more serious than flu), and one looks forward with more hope of an annual inoculation allowing us to resume a more normal life by the end of 2021.

2 thoughts on “The end of the beginning* – Coronavirus”